
Imaging
Those who care for patients with pulmonary, critical care or sleep disorders rely heavily on chest radiology and pathology to determine diagnoses. The Southwest Journal of Pulmonary, Critical Care & Sleep publishes case-based articles with characteristic chest imaging and related pathology.
The editor of this section will oversee and coordinate the publication of a core of the most important chest imaging topics. In doing so, they encourage the submission of unsolicited manuscripts. It cannot be overemphasized that both radiologic and pathologic images must be of excellent quality. As a rule, 600 DPI is sufficient for radiographic and pathologic images. Taking pictures of plain chest radiographs and CT scans with a digital camera is strongly discouraged. The figures should be cited in the text and numbered consecutively. The stain used for pathology specimens and magnification should be mentioned in the figure legend. Those who care for patients with pulmonary, critical care or sleep disorders rely heavily on chest radiology and pathology to determine diagnoses. The Southwest Journal of Pulmonary, Critical Care & Sleep publishes case-based articles with characteristic chest imaging and related pathology. The editor of this section will oversee and coordinate the publication of a core of the most important chest imaging topics. In doing so, they encourage the submission of unsolicited manuscripts. It cannot be overemphasized that both radiologic and pathologic images must be of excellent quality. As a rule, 600 DPI is sufficient for radiographic and pathologic images. Taking pictures of plain chest radiographs and CT scans with a digital camera is strongly discouraged. The figures should be cited in the text and numbered consecutively. The stain used for pathology specimens and magnification should be mentioned in the figure legend.
June 2023 Medical Image of the Month: Solitary Fibrous Tumor of the Pleura
 Figure 1. Posterior to anterior ultrasound image of the lower left hemithorax (A) captured during a therapeutic left-sided thoracentesis. There is a bilobed pedunculated mass (*) attached to the left lower lobe which was not noticed at the time of the procedure, but was identified in retrospect after the mass was discovered on CT. Sagittal reconstruction (B) from a 17-FDG PET-CT also demonstrate the bilobed left lower lobe mass (*). The mass demonstrates diffuse low-level FDG update suggesting relatively low metabolic activity. The appearance of the mass is very similar compared to the image capture from the thoracentesis.
Figure 1. Posterior to anterior ultrasound image of the lower left hemithorax (A) captured during a therapeutic left-sided thoracentesis. There is a bilobed pedunculated mass (*) attached to the left lower lobe which was not noticed at the time of the procedure, but was identified in retrospect after the mass was discovered on CT. Sagittal reconstruction (B) from a 17-FDG PET-CT also demonstrate the bilobed left lower lobe mass (*). The mass demonstrates diffuse low-level FDG update suggesting relatively low metabolic activity. The appearance of the mass is very similar compared to the image capture from the thoracentesis.
 Figure 2. Axial (A) and sagittal oblique (B) reconstructions from a contrast-enhanced chest CT demonstrates a large, heterogeneously enhancing bilobed mass (*) arising from, and connected to the posterior left lower lobe via a small vascular pedicle (arrow).
Figure 2. Axial (A) and sagittal oblique (B) reconstructions from a contrast-enhanced chest CT demonstrates a large, heterogeneously enhancing bilobed mass (*) arising from, and connected to the posterior left lower lobe via a small vascular pedicle (arrow).
 Figure 3. High-powered H & E stain (A) from surgical pathology specimen demonstrates a haphazard arrangement of spindled and ovoid cells with relatively featureless architecture. Other slides demonstrated variable myxoid stroma and areas of dilated, branching “staghorn” vessels. The cells stain strongly positive for CD34 (B) consistent with solitary fibrous tumor of the pleura.
Figure 3. High-powered H & E stain (A) from surgical pathology specimen demonstrates a haphazard arrangement of spindled and ovoid cells with relatively featureless architecture. Other slides demonstrated variable myxoid stroma and areas of dilated, branching “staghorn” vessels. The cells stain strongly positive for CD34 (B) consistent with solitary fibrous tumor of the pleura.
An 85-year-old man presented to our institution for a second opinion and for management of a recurrent left-sided pleural effusion. The patient has a history of CLL, which was diagnosed with a chest wall biopsy 4 years prior to presentation. Since that time, he has undergone chemotherapy and had a good response. In the past 18 months, the patient has had their left-sided pleural effusion drained 24 times. The patient also has a history of hypothyroidism and has had a cholecystectomy.
The patient brought multiple outside imaging studies with him for review. An image capture from a recent ultrasound-guided left thoracentesis (Figure 1A) demonstrated, in retrospect, a pedunculated left lower lobe mass. An outside PET-CT (Figure 1B) was also available, confirming the presence of this mass, which had relatively uniform, low level FDG uptake such that it evade notice on first interpretation. A CT angiogram (Figure 2) demonstrated a large, bilobed mass with heterogeneous arterial enhancement that was attached to and arising from the visceral pleura of the left lower lobe. The angiographic scanning phase demonstrated a well-developed vascular pedicle by which the mass attached to the left lower lobe. Needle biopsy (and subsequent resection) of the mass revealed a 13.5 cm solidary fibrous tumor of the pleura.
Solitary fibrous tumor of the pleura (SFTP) was first described by Klemperer and Rabin in 1931 and has undergone multiple name changes over the years, having been called benign mesothelioma, localized mesothelioma, solitary fibrous mesothelioma, pleural fibroma, submesothelial fibroma, subserosal fibroma, and localized fibrous tumor at various points in the past (1). SFTP is a rare tumor, accounting for less than 5% of tumors arising from the pleura (2). Although it can rarely arise outside the pleura (peritoneum, pericardium, meninges), it most commonly arises from the pleura. It can arise from either the visceral or parietal pleural layer and tends to have a pedunculated attachment in the case of the former with a more broad-based attachment in the case of the later (3). In the case of a SFTP arising from the visceral pleura, it’s pedunculated nature may result in a “wandering” chest mass (4).
SFTP most commonly presents incidentally, often on an imaging study. Imaging findings can be relatively nonspecific, aside from pleural origin. Probably the most salient lesson from this case is to be sure to be sure to perform a diagnostic analysis of any imaging obtained for procedural guidance. SFTP’s are probably best known for the two unusual clinical syndromes that have been described in association with them. There may be hypertrophic pulmonary osteoarthropathy (Pierre-Marie-Bamberg syndrome), which is caused by osteolysis related to the excessive release of hyaluronic acid. There may also refractory hypoglycemia (Doege-Potter syndrome), which is caused by release of insulin-like growth factor II by the tumor cells (4).
Clinton Jokerst MD, Matthew Stib MD, Carlos Rojas MD, Kristopher Cummings MD, Eric Jensen MD, Prasad Panse MD, and Michael Gotway MD
Department of Radiology, Mayo Clinic Arizona, Scottsdale, AZ USA
References
- Klemperer P, Rabin CB. Primary neoplasm of the pleura: a report of five cases. Arch Pathol. 1931;11:385-412.
- Shields TW. Localized fibrous tumors of the pleura. In: Shields TW, ed. General Thoracic Surgery. 4th ed. Baltimore, Md: Williams & Wilkins; 1994
- Robinson LA. Solitary fibrous tumor of the pleura. Cancer Control. 2006 Oct;13(4):264-9. [CrossRef] [PubMed]
- Bhardwaj H, Lindley S, Bhardwaj B, Carlile PV, Huard DR. Catch me if you can: a wandering solitary fibrous tumor of the pleura. Am J Respir Crit Care Med. 2014 Aug 1;190(3):e7-9. [CrossRef] [PubMed]
- Luciano C, Francesco A, Giovanni V, Federica S, Cesare F. CT signs, patterns and differential diagnosis of solitary fibrous tumors of the pleura. J Thorac Dis. 2010 Mar;2(1):21-5. [PubMed]
May 2023 Medical Image of the Month: Methamphetamine Inhalation Leading to Cavitary Pneumonia and Pleural Complications
 Figure 1. Two axial images from a thoracic CT angiogram with intravenous contrast upon admission demonstrates ground-glass opacities in the left upper and bilateral lower lobes.
Figure 1. Two axial images from a thoracic CT angiogram with intravenous contrast upon admission demonstrates ground-glass opacities in the left upper and bilateral lower lobes.
 Figure 2. Axial images from noncontrast CT 19 days later show progression with necrosis and cavitation with areas of pleural dehiscence and loculated hydropneumothorax formation.
Figure 2. Axial images from noncontrast CT 19 days later show progression with necrosis and cavitation with areas of pleural dehiscence and loculated hydropneumothorax formation.
A 31-year-old man with a self-reported history significant for active methamphetamine and OxyContin use (last use of methamphetamine the same day with confirmation on urine drug screen) presented to the hospital with several hours of dyspnea. Having gone into cardiac arrest shortly after, he received several rounds of epinephrine and CPR and was intubated before spontaneous circulation returned. Bedside ultrasound revealed global hypokinesis with left ventricular ejection fraction of 10 to 15%, trivial pericardial effusion, and a moderate left pleural effusion. Chest CT (Figure 1) revealed segmental to subsegmental pulmonary emboli in the left lower lobe and ground-glass opacities in the left upper and bilateral lower lobes. He was treated as septic shock with Vancomycin and Cefepime, eventually speciating methicillin-sensitive Staphylococcus aureus in respiratory culture. Due to difficulty liberating the patient from the ventilator, he underwent tracheostomy tube placement. Chest x-ray on hospital day 18 showed a large left partially loculated hydropneumothorax, for which a left thoracostomy tube was placed. The next day repeat CT chest without contrast (Figure 2) showed persistent moderate left lung volume loss with tethering of the lateral and separate anterior margin of the left upper lobe to the costal pleural margin. A dense consolidation of the left lung base had progressed to developing irregular cavitary spaces with air-fluid level. There was a dehiscence of the cavitary space with the posterior left pleura. The right upper lobe showed extensive tree-in-bud ground-glass opacities and consolidation. The right lower lobe showed necrosis with intrapulmonary cavitary spaces/air-fluid levels. There was associated focal dehiscence of the parenchyma along the posterior cavity with the pleura. Patient had developed bilateral cavitary lung lesions with persistent bilateral hydropneumothoraces.
Typical findings of amphetamine induced lung injury can include ground-glass opacities as seen here. Worldwide prevalence of amphetamine use ranged between 0.3-1.3% for those aged 15-64 in 2009 (1). Crystal meth refers to the pure form of d-methamphetamine hydrochloride that can be smoked and inhaled as heated vapor as well. It can also be administered intravenously. Other amphetamines include MDMA, methyl methcathinone (commonly referred to as bath salts), and methylenedioxyamphetamine. Neural catecholamine reuptake is blocked, and neurotransmitter is expunged into the synaptic cleft. Additionally, serotonin and dopamine reuptake blockade and increased release take place.
With inhalation, there is higher percentage uptake, faster peak time, and slower clearance in the lungs compared to other organs as evidence by data from positron emission tomography. Time to peak concentration is the same between inhalation and intravenous use. Laboratories that produce amphetamines in the United States of America reduce L-ephedrine or D-pseudoephedrine either over red phosphorous with hydrochloric acid or with liquid ammonia and lithium. Therefore, they pose risks of contamination. Red phosphorous is flammable and causes smoke inhalation injury. Other solvents used also contribute to respiratory illness including pulmonary edema and mucous membranes irritation (1).
Typical respiratory symptoms from illicit drug use, including amphetamine use, include dyspnea, cough, dark sputum, and chest pain. Mechanisms include toxic effects on the respiratory system, coronary artery constriction, and impaired coronary artery oxygen delivery leading to chest pain. Dyspnea is a primarily a result of ventilation-perfusion mismatch from vasospasm. Bronchospasm is precipitated by airway mucosal irritation. Mucosal ulceration and burns as well as subsequent diffuse alveolar capillary injury lead to hemoptysis. Cardiogenic pulmonary edema stems from the same causes of chest pain as well as acute hypertension and myocardial ischemia. Noncardiogenic pulmonary edema is a result of alveolar epithelial and endothelial damage.
As compared to cocaine, amphetamines have lower rates of barotrauma including pneumothorax, pneumopericardium, and pneumomediastinum, however these are still significant. There have been reports of MDMA-related epidural pneumatosis and retropharyngeal emphysema (1). Air dissects along fascial planes when alveoli are injured and travels up the pulmonary vascular sheath into the mediastinum, pericardium, and between the parietal and visceral layers. When inhaled, coughing, and performing a Valsalva maneuver predispose the patient to this complication (2). Additionally, pneumothorax is more common with exertion shortly after consumption. Attempts at intravenous administration along the chest, supraclavicular regions, and internal jugular veins increase risk of pneumothorax (3). Hemothorax and pseudoaneurysm have been documented as well (2).
Kia Ghiassi DO1, Colin Jenkins MD1, Prateek Juneja DO2
1,2University of California Riverside, Riverside, CA USA
2Inspira Health, Vineland, NJ USA
References
- Tseng W, Sutter ME, Albertson TE. Stimulants and the lung : review of literature. Clin Rev Allergy Immunol. 2014 Feb;46(1):82-100. [CrossRef] [PubMed]
- Nguyen ET, Silva CI, Souza CA, Müller NL. Pulmonary complications of illicit drug use: differential diagnosis based on CT findings. J Thorac Imaging. 2007 May;22(2):199-206. [CrossRef] [PubMed]
- Gotway MB, Marder SR, Hanks DK, et al. Thoracic complications of illicit drug use: an organ system approach. Radiographics. 2002 Oct;22 Spec No:S119-35. [CrossRef] [PubMed]
March 2023 Medical Image of the Month: Spontaneous Pneumomediastinum as a Complication of Marijuana Smoking Due to Müller's Maneuvers

Figure 1. PA chest radiograph obtained at the time of admission (A) demonstrating gas densities (arrows) along left heart border, left paratracheal stripe, upper mediastinum and neck extending into the right supraclavicular fossa in keeping with pneumomediastinum. Follow-up PA chest radiograph performed just before discharge (B) demonstrates resolution of pneumomediastinum.

Figure 2. Two axial images through the anterior mediastinum obtained from a contrast-enhanced chest CT demonstrating gas densities (arrows) in the mediastinum anterior to the heart and around the esophagus in-keeping with pneumomediastinum.
A 35-year-old woman with a medical history notable for celiac disease, ulcerative colitis, and bipolar disorder presents to the Emergency Department for evaluation of a strange sensation in the chest and neck associated with nausea and vomiting for one day. The patient also reports persistent nausea and markedly decreased oral intake for the last four days. She reported no concomitant symptoms such as shortness of breath, wheezing, fever, or chills. She denies diarrhea or constipation. Socially, she admits to smoking marijuana daily, and alcohol occasionally.
Vital sign shows blood pressure 147/97 mmHg, pulse 92 BPM, temperature 37.3°C, SpO2 96% breathing ambient air. She appears nontoxic and well-nourished, and the lungs are clear to auscultation bilaterally without any wheezes, rales, or rhonchi. The heart examination reveals a regular rate and rhythm, with normal S1 and S2 heart sounds and no murmurs, rubs, or gallops. The abdomen is soft, non-tender, and not distended. Her extremities do not exhibit any clubbing, cyanosis, or edema. CBC and CMP were unremarkable, and the drug screen test was positive for THC. An ECG is obtained (not shown here), which reveals a normal sinus rhythm with a heart rate of 55 beats/min and no ST-segment or T-wave abnormalities. Chest x-ray and CTA chest, CT abdominal with oral contrast were obtained (Figures 1 and 2). Upon further questioning of the patient’s social history, it was discovered that she smokes marijuana daily using water pipes, and while utilizing a water pipe she attempted a full inspiration against a closed mouth and nose, a technique known as the Müller’s maneuver.
Spontaneous pneumomediastinum (SPM) is a rare condition in which air escapes from the lungs and collects in the mediastinum, the space between the lungs. SPM is almost always a benign, self-limited condition. While SPM can be caused by a variety of factors, including coughing, vomiting, and physical trauma, this case report presents a rare instance of SPM caused by marijuana smoking. Spontaneous pneumomediastinum (SPM) was reported in 1939 by Johns Hopkins clinician Louis Hamman for whom the Hamman sign is named. It is defined as free air or gas contained within the mediastinum, which almost originates from the alveolar space or the conducting airways. Many authors distinguish spontaneous pneumomediastinum as a form of pneumomediastinum that is not associated with blunt force or penetrating chest trauma, endobronchial or esophageal procedures, neonatal lung disease, mechanical ventilation, chest surgery, or other invasive procedures.
The mechanism by which marijuana smoking leads to pneumomediastinum is not well understood, but it is thought to involve increased intra-alveolar pressure and alveolar rupture. This can result in the escape of air into the mediastinum, leading to the development of pneumomediastinum. SPM has been associated with the inhalation of drugs such as cocaine, amphetamines, and marijuana (1-4). Attempted inspiration through a closed glottis or Muller’s maneuver results in a drop in intrathoracic pressure, which increases alveolar air volume, causing alveolar distension and rupture which can cause shear damage and air leakage along a bronchovascular bundle into the mediastinum.
The patient, in this case, was a 35-year-old woman with a history of marijuana smoking who presented with symptoms of chest pain, shortness of breath, and dysphagia. Physical examination revealed subcutaneous emphysema and a chest x-ray confirmed the presence of SPM. This case highlights the potential respiratory complications associated with marijuana smoking, which can lead to SPM and other adverse outcomes. While marijuana use is becoming increasingly common and accepted, it is important for healthcare providers to be aware of the potential risks and to educate their patients about the potential consequences of marijuana use. Further research is needed to understand the full extent of the respiratory effects of marijuana smoking and to develop appropriate interventions and treatments.
Mohammad Abdelaziz Mahmoud DO
Doctors Medical Center of Modesto and Emanuel Medical Center
Modesto and Turlock, CA USA
References
- Weiss ZF, Gore S, Foderaro A. Pneumomediastinum in marijuana users: a retrospective review of 14 cases. BMJ Open Respir Res. 2019 Feb 12;6(1):e000391. [CrossRef] [PubMed]
- Al-Mufarrej F, Badar J, Gharagozloo F, Tempesta B, Strother E, Margolis M. Spontaneous pneumomediastinum: diagnostic and therapeutic interventions. J Cardiothorac Surg. 2008 Nov 3;3:59. [CrossRef] [PubMed]
- Puri C, Rhee K, Harish VK, Slack D. Marijuana induced spontaneous pneumomediastinum. J Community Hosp Intern Med Perspect. 2021 Jun 21;11(4):516-517. [CrossRef] [PubMed]
- Motes A, Laoveeravat P, Thongtan T, Nugent K, Islam S, Islam E. Marijuana use-induced spontaneous pneumomediastinum. Proc (Bayl Univ Med Cent). 2020 Dec 7;34(2):274-275. [CrossRef] [PubMed]
Cite as: Mahmoud MA. March 2023 Medical Image of the Month: Spontaneous Pneumomediastinum as a Complication of Marijuana Smoking Due to Müller's Maneuvers. Southwest J Pulm Crit Care Sleep. 2023;26(3):31-33. doi: https://doi.org/10.13175/swjpccs058-22 PDF
December 2022 Medical Image of the Month: Bronchoesophageal Fistula in the Setting of Pulmonary Actinomycosis

Figure 1. Axial (A) and sagittal (B) reconstructions from a contrast-enhanced chest CT demonstrates an ill-defined low-attenuation subcarinal mass (*) which causes deformity of the left mainstem bronchus (LMSB) (arrow). Axial reconstruction from a repeat contrast-enhanced CT performed 6 days later (C) demonstrates a gas-filled fistulous tract between the LMSB and esophagus through the mass (arrowheads). An esophogram (D) performed 24 hours after esophageal stent placement demonstrates occlusion of the fistula.
A 65-year-old woman, never smoker with hypothyroidism, hypertension, anxiety, and depression disorders, initially presented to the emergency department with progressive nonspecific chest discomfort for two days. She had CT Angio, which was negative for PE but showed a 4.6 cm subcarinal centrally necrotic nodal mass (Figure 1A-B). She was subsequently advised to follow up with her primary care physician. A week later, she attended our emergency department again with a new intermittent cough and one episode of non-bloody emesis. She reported a sensation of drowning with the intake of liquids and subsequent intractable coughing. Otherwise, she did not have other associated symptoms such as shortness of breath, abdominal pain, fever, sweats, or chills.
Vital signs and physical exam were unremarkable. A repeat chest CT was performed, which demonstrated internal cavitation of the subcarinal mass with fistulous communication between the lumen of the midthoracic esophagus and the proximal left mainstem bronchus posteriorly, suggestive of broncho-esophageal fistula (Figure 1C). She subsequently underwent bronchoscopy, which revealed areas of friable bronchial mucosal nodularity along the posterior membrane of the mid to distal left mainstem bronchus. Despite a thorough airway inspection, no clear fistula was observed, and no gastric or bilious material was seen within the airway. She underwent endobronchial ultrasound (EBUS) with transbronchial nodal aspiration (TBNA) of the mediastinal lymphadenopathy, which showed extensive necrotic debris and granulomatous inflammation; however, Giemsa stain was negative and no sulfur granules were observed. An upper endoscopy was performed in tandem with the bronchoscopy. The EGD identified a cratered esophageal ulcer in the mid esophagus, which was biopsied. As well, a 25 mm fistulous track was found within the ulcerated region, and thus, an esophageal stent was placed. An esophagogram performed the next day showed no evidence of a leak (Figure 1D), which is suggestive of successful occlusion of the fistula. The esophageal biopsy was negative for malignancy though it also revealed ulcerated squamous mucosa with marked acute and chronic inflammation with reactive granulation tissue.
Infectious workup included Legionella urinary antigen, Streptococcus pneumoniae urinary antigen, MRSA nasal screen, serum Aspergillus antigen, coccidiomycosis IgG/IgM (by EIA and CF/ID), QuantiFERON TB gold, and beta-D-glucan, all of which were negative. Histoplasma urinary antigen, Histoplasma and Blastomyces serum antibodies were also negative. Anaerobic cultures from lymph node aspirate later grew Actinomycetes.
Infectious disease was consulted, and the patient was started on ceftriaxone 2 g IV daily for three weeks, for pulmonary actinomyces infection, with a plan to transition to oral amoxicillin 750 mg three times a day for six months. She had a clinic follow-up appointment in eight weeks, in which she reported complete resolution of her symptoms.
Actinomycetes are branching gram-positive anaerobic bacteria and rarely cause infection, with only about 1 in 300,000 cases reported per year (1). Infections can involve any organ system, with pulmonary actinomycosis being the third most common location, representing around 15 % of the total disease cases (2). Actinomyces species are part of normal flora found in the mouth and gastrointestinal tract; therefore, it is hypothesized that pulmonary actinomycosis is caused by aspiration (3).
Diagnosis by clinical features alone can be challenging as it shares many symptoms associated with chronic infections like a low-grade fever, sputum production, cough and malaise. Therefore, it may be wrongfully diagnosed as tuberculosis, lung abscess and fungal infection. It can also often be confused with malignancy. Mabeza et al. (4) reported that around a quarter of cases with thoracic actinomyces were initially thought to have carcinoma.
Image findings of pulmonary actinomyces are also quite diverse. A retrospective study of 94 patients diagnosed with pulmonary actinomycosis pathologically over ten years in Korea revealed that the most common chest CT finding was consolidation (74.5%), mediastinal or hilar lymph node enlargement (29.8%), atelectasis (28.7%), cavitation (23.4%), ground-glass opacity (14.9%), and pleural effusion (9.6%) (5). Actinomyces can spread from the lung to the pleura, mediastinum, and chest wall. It is hypothesized that the mechanism behind their ability to travel through these anatomical barriers is due to their ability to produce proteolytic enzymes (6). Given its indolent presentation, proper diagnosis and treatment may be delayed leading to the involvement of adjacent structures and potentially life-threatening complications, including massive hemoptysis or bronchoesophageal fistula formation.
Detection of ‘sulfur’ granules histologically has been previously described as the hallmark for the diagnosis; however, they can also be found in other infections like nocardiosis (7), and they are only observed in 50% of cases; therefore, their absence does not exclude actinomycosis. Culture confirmation is typically clinically difficult because of inadequate anaerobic conditions, prior antibiotic therapy, or overgrowth of concomitant organisms (2).
The principal treatment for pulmonary actinomycosis has been penicillin; however, there are no well-established guidelines regarding the duration of antibiotic therapy. High-dose intravenous penicillin is usually used for four to six weeks, followed by six to twelve months of oral amoxicillin in most cases (9). Surgery is typically reserved for pulmonary actinomycosis complicated by abscesses, empyemas, discharging fistulas and sinuses, life-threatening hemoptysis, exclusion of malignancy, and for patients who do not respond to antibiotic therapies (10).
John Fanous MD1, Nikita Ashcherkin MD2, Michael Gotway MD3, Kenneth Sakata, MD1 and Clinton Jokerst MD3
Division of Pulmonology1, Department of Internal Medicine2, and Department of Radiology3
Mayo Clinic Arizona, Scottsdale, AZ USA
References
- Gajdács M, Urbán E, Terhes G. Microbiological and Clinical Aspects of Cervicofacial Actinomyces Infections: An Overview. Dent J (Basel). 2019 Sep 1;7(3):85. [CrossRef] [PubMed]
- Han JY, Lee KN, Lee et al. An overview of thoracic actinomycosis: CT features. Insights Imaging. 2013 Apr;4(2):245-52. [CrossRef] [PubMed]
- Park HJ, Park KH, Kim SH, Sung H, Choi SH, Kim YS, Woo JH, Lee SO. A Case of Disseminated Infection due to Actinomyces meyeri Involving Lung and Brain. Infect Chemother. 2014 Dec;46(4):269-73. [CrossRef] [PubMed]
- Mabeza GF, Macfarlane J. Pulmonary actinomycosis. Eur Respir J. 2003 Mar;21(3):545-51. [CrossRef] [PubMed]
- Kim SR, Jung LY, Oh IJ, et al. Pulmonary actinomycosis during the first decade of 21st century: cases of 94 patients. BMC Infect Dis. 2013 May 14;13:216. [CrossRef] [PubMed]
- Heo SH, Shin SS, Kim JW, Lim HS, Seon HJ, Jung SI, Jeong YY, Kang HK. Imaging of actinomycosis in various organs: a comprehensive review. Radiographics. 2014 Jan-Feb;34(1):19-33. [CrossRef] [PubMed]
- Brown JR. Human actinomycosis. A study of 181 subjects. Hum Pathol. 1973 Sep;4(3):319-30. [CrossRef] [PubMed]
- Zhang AN, Guss D, Mohanty SR. Esophageal Stricture Caused by Actinomyces in a Patient with No Apparent Predisposing Factors. Case Rep Gastrointest Med. 2019 Jan 2;2019:7182976. [CrossRef] [PubMed]
- Valour F, Sénéchal A, Dupieux C, et al. Actinomycosis: etiology, clinical features, diagnosis, treatment, and management. Infect Drug Resist. 2014 Jul 5;7:183-97. [CrossRef] [PubMed]
- LoCicero J 3rd, Shaw JP, Lazzaro RS. Surgery for other pulmonary fungal infections, Actinomyces, and Nocardia. Thorac Surg Clin. 2012 Aug;22(3):363-74. [CrossRef] [PubMed]
November 2022 Medical Image of the Month: COVID-19 Infection Presenting as Spontaneous Subcapsular Hematoma of the Kidney

Figure 1. Enhanced abdominal CT images in the axial (A) and coronal (B) reconstruction planes show uniform high attenuation material surrounding the right kidney but conforming to renal shape consistent with subcapsular hematoma (arrows). Note the reactive perinephric stranding in the right retroperitoneal space.
A 57-year-old woman with pertinent medical history of hypertension presented to the emergency department with 3 days of right sided lower abdominal pain radiating to the flank, associated with nausea and nonbloody, nonbilious emesis. She reported recent travel to Florida where she visited amusement parks, but only rode small children’s rides with no experienced physical trauma. She experienced fatigue and chills 5 days prior to presentation and tested positive for SARS-CoV2 virus on admission. She had been vaccinated for COVID-19 x3 (Moderna). No other significant history nor medications were noted, and review of systems was otherwise unremarkable.
Urinalysis demonstrated mild ketonuria (20), proteinuria (100) and moderate hematuria on urinalysis while BUN and creatinine remained stable at baseline throughout. Physical examination confirmed costovertebral angle tenderness to the right side. CT abdomen revealed an American Association for the Surgery of Trauma (AAST) grade 3 right renal subcapsular hematoma with 2.1 cm laceration and striations with a pre-existing right arterial aneurysm. Care was escalated to ICU for closer renal function monitoring; urology and nephrology were consulted for suspected ischemic nephropathy and renal compression with concern for Page (external compression) kidney . After exclusion of traumatic and known causes, interdisciplinary discussion came to the consensus of COVID-19 infection induced SRH.
Subcapsular renal hematoma (SRH) is a challenging medical condition in which hematoma formation may exert pressure on surrounding parenchyma resulting in hypoperfusion or ischemia, with overt concern for rupture with subsequent hemorrhage and hemodynamic instability. While this is a predominantly a medical condition precipitated by neoplasms, abdominal trauma or anticoagulant use, sporadic cases of SRH have been observed since the onset of the COVID-19 pandemic. Here, we present a rare case and imaging of COVID-19 infection induced SRH.
Even three years since the start of the COVID-19 pandemic, clinicians continue to unravel COVID-19’s impact on various body systems. While renal involvement is observed in the form of acute kidney injury in over 30% of hospitalized COVID-19 patients (1), SRH has rarely been documented. Retroperitoneal bleeding from various organs has occurred in COVID-19 patients, but this bleeding is often secondary to prophylactic anticoagulation to combat the suspected inflammation-induced hypercoagulable state (2-4). Seldom does retroperitoneal bleeding occur in the absence of anticoagulant use or other precipitating cause, as is seen in our patient with SRH. Tavoosian et al. (5) illustrate a similar case of an otherwise healthy, COVID-19 positive individual that developed spontaneous subcapsular renal hematoma without history of malignancy, trauma or anticoagulant use. The mechanism by which spontaneous SRH may occur in COVID-19 patients is still unclear. However, our case adds to literature another presentation of spontaneous SRH caused by COVID-19 infection with unique imaging findings and add to the growing differential for causes of SRH and the differential of abdominal pain.
Kally Dey1, Shil Punatar DO2, Tauseef Sarguroh MD2
1 Midwestern University Chicago College of Osteopathic Medicine, Downers Grove, IL USA
2 Franciscan Health Olympia Fields, Olympia Fields, IL USA
References
- Hirsch JS, Ng JH, Ross DW, et al. Acute kidney injury in patients hospitalized with COVID-19. Kidney Int. 2020;98(1):209-218. [CrossRef] [PubMed]
- Patel I, Akoluk A, Douedi S, et al. Life-Threatening Psoas Hematoma due to Retroperitoneal Hemorrhage in a COVID-19 Patient on Enoxaparin Treated With Arterial Embolization: A Case Report. J Clin Med Res. 2020;12(7):458-461. [CrossRef] [PubMed]
- Cattaneo M, Bertinato EM, Birocchi S, et al. Pulmonary Embolism or Pulmonary Thrombosis in COVID-19? Is the Recommendation to Use High-Dose Heparin for Thromboprophylaxis Justified?Thromb Haemost. 2020;120(8):1230-1232. [CrossRef][PubMed]
- Zhou F, Yu T, Du R, et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study. Lancet. 2020 Mar 28;395(10229):1054-1062. Erratum in: Lancet. 2020 Mar 28;395(10229):1038.[CrossRef] [PubMed]
- Tavoosian A, Ahmadi S, Aghamir SMK. Spontaneous perirenal haematoma (SPH) in a COVID-19 patient: A rare case report. Urol Case Rep. 2022 May;42:102006.[CrossRef] [PubMed]
Cite as: Dey K, Punatar S, Sarguroh T. November 2022 Medical Image of the Month: COVID-19 Infection Presenting as Spontaneous Subcapsular Hematoma of the Kidney. Southwest J Pulm Crit Care Sleep. 2022;25(4):67-68. doi: https://doi.org/10.13175/swjpccs041-22 PDF
November 2022 Imaging Case of the Month: Out of Place in the Thorax
Department of Radiology, Mayo Clinic, Arizona
5777 East Mayo Boulevard
Phoenix, Arizona USA
History of Present Illness: A 30-year-old woman presented with complaints of left-sided back pain and numbness. She denied any history of trauma.
PMH, SH, FH: No significant past medical history. She denied smoking and use of illicit substances. Her family history was largely unremarkable, positive only for a history of gastrointestinal stromal tumor affecting her father.
Medications: Her medications included fluoxetine, spironolactone, and Celebrex (celecoxib).
Physical Examination: The patient’s physical examination showed her to be afebrile with pulse rate and blood pressure within the normal range.
Laboratory Evaluation: A complete blood count showed a hemoglobin and hematocrit value of 14.3 gm/dL (normal, 13.2-16.6 gm/dL) and 41.5% (normal, 38.3-48.6%) and a platelet count of 253 x x109/L (normal, 135-317 x109/L). The white blood cell count was normal at 6.9 x109/L (normal, 3.4-9.6 x109/L), with no left shift. The eosinophil count was normal. Liver function studies were entirely normal. Serum chemistries were completely within normal limits aside from a minimally elevated serum calcium level of 10.1 mg/dL (normal, 6.6-10 mg/dL).
Frontal chest radiography (Figure 1) was performed.

Figure 1. Frontal chest radiography shows normal heart size, clear lungs, no evidence of pleural effusion or peribronchial or mediastinal lymph node enlargement.
Which of the following represents an appropriate interpretation of the frontal chest and lateral radiograph? (Click on the correct answer to be directed to the second of 11 pages)
- Frontal chest radiography shows normal findings
- Frontal chest radiograph shows numerous small nodules
- Frontal chest radiography shows rib abnormalities
- None of the above
- More than one of the above
Cite as: Gotway MB. November 2022 Imaging Case of the Month: Out of Place in the Thorax. Southwest J Pulm Crit Care Sleep. 2022;25(5):61-66. doi: https://doi.org/10.13175/swjpcc049-22 PDF
October 2022 Medical Image of the Month: Infected Dasatinib Induced Chylothorax-The First Reported Case

Figure 1. Upright PA chest radiograph (A) demonstrates a large left-sided pleural effusion with some lateral fluid suggesting loculation. Bedside ultrasound to guide thoracentesis (B) demonstrates multiple loculations within the effusion (arrowheads). Thoracentesis yielded 2 liters of milky white fluid (C).

Figure 2. Axial lung window (A) and soft tissue window (B) reconstructions from a chest CT with intravenous contrast performed following thoracentesis demonstrates a circumferential irregular left-sided pleural effusion with air space disease within the left lower lobe concerning for infection. A simple-appearing right-sided effusion is noted as well (*).
Case Report
A 45-year-old man with chronic myeloid leukaemia (CML) on dasatinib presented to the emergency department with a 2-week history of dry cough, worsening shortness of breath and left-sided chest pain that had worsened on the day of presentation. On examination, oxygen saturation was 98% on 2 L nasal cannula, respiratory rate 22 bpm, pulse 77 bpm, blood pressure 117/90 mmHg and his temperature was 37.9° C (100.2 F). Examination of the left chest showed no air entry and stony dull percussion note.
Laboratory results were significant for leucocytosis with a neutrophil count of 11.2, elevated CRP of 414, mildly elevated lactate of 1.1. Initial chest X-ray showed large left-sided pleural effusion and a small volume right effusion (Figure 1A). The patient was started on IV piperacillin /tazobactam, blood cultures were obtained and the dasatinib was held.
Ultrasound-guided left thoracentesis and drain placement was performed, on ultrasound the effusion demonstrated several loculations (Figure 1B). An 18Fr drain was inserted and 2L of white purulent/milky material fluid was drained (Figure 1C). Pleural fluid analysis showed abundant neutrophils, macrophages, lymphocytes and a few reactive mesothelial cells. Cytological analysis was negative for malignant cells. The fluid was exudative by Light’s criteria as total protein was 52.9 g/l and serum protein was 77 g/l with the ratio 0.68. Triglyceride level was 2.0 mmol/l and fluid cholesterol was 1.6 mmol/L indicative of chylothorax.
Over time, pleural cultures were positive for beta haemolytic Strep group C/G sensitive to penicillin G and erythromycin and both fungal and tuberculosis cultures were negative. Blood cultures were negative. Antimicrobial therapy was deescalated to Penicillin G. A subsequent chest CT (following intra-pleural fibrinolytic therapy) showed small left basal effusion with overlying consolidation and no occlusive lesion identified (Figure 2). After 9 days the pleural drain was removed, and the patient had no reaccumulation of their chylothorax. The patient remained clinically well and was discharged after a course of four weeks of antibiotics. At a 2 week follow up the patient was asymptomatic and had a normal physical exam. His inflammatory markers were back to normal CRP was 0.5 and WBC count was 6.5.
Discussion
Chylothorax is accumulation of chyle into the pleural space related to obstruction or disruption of the thoracic duct. It is a rare condition that may arise from diverse etiologies broadly categorized as traumatic or non-traumatic/spontaneous (1). Chylothorax is widely believed to be inherently bacteriostatic, with rare incidence of infected chylous effusions affecting a wide variety of patients with different causative organisms and a mostly benign course (2).
Dasatinib is a second-generation tyrosine kinase inhibitor that is recommended as the first-line therapy for newly diagnosed chronic myeloid leukaemia (CML) or acute lymphoblastic leukaemia (ALL) with positive Philadelphia chromosome (Ph+) or as an alternative for the failure of prior therapy for CML. Dasatinib is known to cause fluid retention which commonly presents as an exudative pleural effusion (3), chylothorax is rarely seen with 7 cases in total related to dasatinib use were published in the literature (4).
This is the first reported case of infected chylothorax among the population using dasatinib. Infected chylothorax in general is rare, affecting wide variety of patients with different organisms and mostly benign course (2). In this report the patient was stable on presentation and showed good response to antibiotics, chest drainage, holding of dasatinib and dietary fat restriction. Given the loculated appearance of the fluid the patient benefited from a dose of thrombolysis, which was reported as an option in such a scenario (5).
In patients with CML on dasatinib presenting with pleural effusion, the medication should be considered as one of the possible causes. Furthermore, infected chylothorax should be considered in the deferential diagnosis as a source of sepsis in patients presenting with a sepsis-like clinical picture and pleural effusion. The case also reflects the importance of bedside ultrasound in both clinically examining the patients and as a guide for thoracentesis and guidance for therapy.
Mortada Mohammed1 MD MRCPI, Mohanad Abdelrahim2 MD, Keshav Sharma3 MD MRCPI
1Respiratory medicine registrar Wexford General Hospital, Wexford, Ireland
2Medical Senior House officer Wexford General Hospital, Wexford, Ireland
3Consultant Respiratory and General Medicine Physician, Wexford General Hospital, Wexford, Ireland
References
- McGrath EE, Blades Z, Anderson PB. Chylothorax: aetiology, diagnosis and therapeutic options. Respir Med. 2010 Jan;104(1):1-8. [CrossRef] [PubMed]
- Eubank L, Gabe L, Kraft M, Billheimer D. Infected chylothorax: a case report and review. Southwest J Pulm Crit Care. 2018 Aug 25;17(2):76–84. [CrossRef]
- Keating GM. Dasatinib: A Review in Chronic Myeloid Leukaemia and Ph+ Acute Lymphoblastic Leukaemia. Drugs. 2017 Jan;77(1):85-96. [CrossRef] [PubMed]
- Chen B, Wu Z, Wang Q, Li W, Cheng D. Dasatinib-induced chylothorax: report of a case and review of the literature. Invest New Drugs. 2020 Oct;38(5):1627-1632. [CrossRef] [PubMed]
- Nair SK, Petko M, Hayward MP. Aetiology and management of chylothorax in adults. Eur J Cardiothorac Surg. 2007 Aug;32(2):362-9. [CrossRef] [PubMed]
September 2022 Medical Image of the Month: Epiglottic Calcification
 Figure 1. Lateral (A) and frontal (B) topogram from a neck CT demonstrates linear calcifications in the expected location of the epiglottis (black arrows). Sagittal multiplanar reconstructions demonstrate prominent calcification of the epiglottis (white arrow).
Figure 1. Lateral (A) and frontal (B) topogram from a neck CT demonstrates linear calcifications in the expected location of the epiglottis (black arrows). Sagittal multiplanar reconstructions demonstrate prominent calcification of the epiglottis (white arrow).
In consideration of dysphagia, most cases predominate in the oropharyngeal region with the remainder caused primary by esophageal causes. Lesser known and studied is the development of dysphagia and globus sensation from epiglottic pathology, namely epiglottic calcification. With less than a dozen published cases in literature, very little data exists on identification, diagnosis, and treatment of this known cause of morbidity. Here we present a case of oropharyngeal dysphagia arising from a rare cause, epiglottic calcification.
An 81-year-old man with a history of aortic stenosis and carotid artery stenosis presented with worsening dysphagia over the course of one month. The patient reported significant dysphagia, initially to solids and subsequently to liquids causing a weight loss of over 50 pounds. Physical exam of the oropharynx and neck were unremarkable. A bedside swallow evaluation suggested mildly decreased hyolaryngeal movement, but no other significant abnormalities. A barium swallow study revealed incomplete epiglottic excursion during the pharyngeal phase of swallowing. The patient then underwent evaluation with a contrast-enhanced esophagogram, which showed severe esophageal dysmotility and gastroesophageal reflux. A CT of the neck demonstrated calcification of the epiglottis without epiglottal enlargement. ENT was consulted, the patient underwent flexible fiberoptic laryngoscopy and also EGD with biopsy. No other esophageal or gastric pathology were identified other than the epiglottic calcification. As no effective treatment is known at this time, the patient was changed to a modified diet with ongoing speech and swallow therapy as an outpatient.
Epiglottic calcification is a rare cause of dysphagia that is poorly understood in its etiology, clinical course and outcome (1). This case demonstrates that despite consultant team recommendations, no clear evaluation pathway or treatment currently exists. Currently, diagnosis can be accomplished with radiologic evaluation along with exclusion of other causes; however, no definitive treatments are available for this rare condition. Although the condition itself is rare, epiglottic calcification should be considered when other more common causes of significant dysphagia are ruled out.
Shil Punatar DO1, Dayoung Song MD1, Azkaa Zaman DO1, Benjamin Jiao DO2, and Tilemahos Spyratos DO1,3
1Department of Internal Medicine, Franciscan Health, Olympia Fields, IL
2Department of Radiology, Franciscan Health, Olympia Fields, IL
3Department of Gastroenterology, Franciscan Health, Olympia Fields, IL
Reference
1. Günbey HP, Günbey E, Sayit AT. A rare cause of abnormal epiglottic mobility and dyspagia: calcification of the epiglottis. J Craniofac Surg. 2014 Nov;25(6):e519-21. [CrossRef[[PubMed]
Medical Image of the Month: An Unexpected Cause of Chronic Cough

Figure 1. Axial image from a contrast-enhanced CT demonstrates a hollow, calcified structure in the bronchus intermedius with thickening suggesting inflammation in the surrounding bronchial wall (arrow).

Figure 2. Photograph of chicken bone fragment retrieved from bronchus intermedius during flexible bronchoscopy (A). In retrospect, this fragment of bone is visible on the topogram from the chest CT (B) and is circled. Note the prominent notch that is visible on CT and on the actual bone fragment (arrowheads).
Sometimes it is as simple as it looks! A previously healthy nonsmoking 40 years old man presented with a 7-month history of dry cough which was misdiagnosed as asthma. He had persistent cough despite appropriate asthma treatment including empiric PPIs. This patient had undergone extensive lab work up and evaluation; from negative viral and fungal panel, repeated pulmonary function tests which were within normal limits, chest x-rays, and CT scans which had shown small local calcification in the bronchus intermedius with significant thickening of the surrounding bronchial wall (Figure 1). The decision was made to proceed with flexible bronchoscopy, which yielded a chicken bone fragment with surrounding granulation tissue as shown in Figure 2A. In retrospect the bone is visible within the bronchus intermedius on the topogram from the CT scan, see Figure 2B.
Foreign body aspiration in adults reported in low rates (0.66 per 100 000) (1). Despite being uncommon, neurological disorders, alcohol abuse, advanced age and altered level of consciousness all found to be the main underlying cause of foreign body aspiration in adults (2). Still, 10% of adult patients with foreign body aspiration have no known risk factors (3). Usually, diagnosis of foreign body aspiration in adults is straightforward only if the patient’s history involves aspiration or choking event. But, if the initial event goes unnoticed, the clinical picture maybe similar to obstructive lung diseases such as COPD or asthma.
Yazan Khair 1, Hussam Al-Jawaldeh2, Ayah AL Mufleh3 , Maxim Abu Joudeh4, Emad Hammode5
1Pulmonary department, Royal Medical Services (RMS), Amman, Jordan
2Internal Medicine Resident, Canyon Vista Medical Center, Sierra Vista, AZ USA
3Internal Medicine transitional program, King Hussein Cancer Center, Amman, Jordan
4Internal Medicine Resident, Canyon Vista Medical Center, Sierra Vista, AZ USA
5Program Director of Canyon Vista Medical Center Internal Medicine program, Sierra Vista, AZ USA
References
- Lund, ME. Foreign body removal in: Ernst A, Herth, FJF eds. Principles and Practice of Interventional Pulmonolgy. New York, NY: Springer; 2013:477-488.
- Singh A, Kaur M. Recurrent pneumonitis due to tracheobronchial foreign body in an adult. JIACM, 2007:8:242-44.
- Mise K, Jurcev Savicevic A, Pavlov N, Jankovic S. Removal of tracheobronchial foreign bodies in adults using flexible bronchoscopy: experience 1995-2006. Surg Endosc. 2009 Jun;23(6):1360-4. [CrossRef] [PubMed]
Cite as: Khair Y, Al-Jawaldeh H, Mufleh A, Joudeh M, Hammode E. Medical Image of the Month: An Unexpected Cause of Chronic Cough. Southwest J Pulm, Crit Care & Sleep. 2022;25(2):23-24. doi: https://doi.org/10.13175/swjpccs032-22 PDF
August 2022 Imaging Case of the Month: It’s All About Location
Department of Radiology
Mayo Clinic, Arizona
5777 East Mayo Boulevard
Phoenix, Arizona 85054
A 78–year–old man with a history of hyperlipidemia, hypertension, paroxysmal atrial fibrillation, and transcatheter aortic valve replacement on anticoagulation presented to the Emergency Room with a 2-month history of cough and exertional shortness of breath. He denied fever, chills, nausea, and chest pain. The patient had undergone three COVID-19 vaccines, the most recent 3 months earlier. He had noted some recent bruising, but denied any recent trauma.
The patient’s past medical history also included a history of prostate carcinoma 10 years earlier treated with radiation therapy. The patient’s past surgical history was remarkable for remote vasectomy, endoscopic sinus surgery and percutaneous aortic valve replacement. He was a former smoker and reported no allergies or illicit drug use; alcohol use was at most moderate, consisting of an occasional beer. The patient’s medications included a statin, warfarin, and metoprolol.
The patient’s physical examination showed normal vital signs and was remarkable only for some decreased breath sounds over the left lower thorax. The patient was afebrile. Bruising was noted involving the right hand and right abdominal wall, but without limitations in range of motion or associated pain.
A complete blood count showed a hemoglobin and hematocrit value of 7.7 gm/dL (normal, 13.2-16.6 gm/dL) and 23.9% (normal, 38.3–48.6%) and a platelet count of <2 x x109/L (normal, 135-317 x109/L). The white blood cell count was minimally abnormal at 9.7 x109/L (normal, 3.4-9.6 x109/L), with a mild left shift with a neutrophil level of 7.11 x109/L (normal, 1.56-6.45 x109/L). The eosinophil count was normal, but reticulocytes were elevated at 4.06% (normal, 0.60-2.71%). The INR was elevated at 2.3, with a prolonged prothrombin time of 25.8 sec (normal, 9.4-12.5 sec). Fibrinogen was also mildly abnormally elevated. Serum chemistries were largely within normal limits, with a mild elevation in lactate dehydrogenase at 273 U/L (normal, 122–222 U/L). Serum iron values were low at 30 mg/dL (normal, 50-150 mg/dL), with the total iron binding capacity abnormally decreased also. An ECG was unremarkable. A serum NT-Pro BNP value was elevated at 1174 pg/mL (normal, ≤122 pg/mL). Liver and renal function were within normal limits.
Frontal and lateral chest radiography (Figure 1) was performed.

Figure 1. Frontal (A) and lateral (B) chest.
Which of the following represents an appropriate interpretation of the frontal chest and lateral radiograph? (Click on the correct answer to be directed to the second of twelve pages)
- Frontal chest radiography shows a large left pleural effusion
- Frontal chest radiograph shows focal right lung opacity
- Frontal chest radiography shows pleural calcification
- Frontal chest radiography shows right peribronchial lymph node enlargement
- More than one of the above
July 2022 Medical Image of the Month: Pulmonary Nodule in the Setting of Pyoderma Gangrenosum (PG)

Figure 1. Unenhanced lung window chest CT images in the axial (A) and sagittal (B) planes show a solid, non-calcified irregular left upper lobe mass (arrow) with spiculated margins. The nodule demonstrates enhancement on soft tissue windows (C) with associated mediastinal adenopathy (arrowhead). The mass and adenopathy are FDG-avid on axial fused PET-CT image (D).

Figure 2. (A) Photograph of one of the patient’s skin lesions. (B) Hematoxylin and Eosin stained low-power pathological image of a biopsy specimen from a skin lesion demonstrates dense mixed neutrophilic dermal inflammation. Extensive infectious and neoplastic workup was negative. The histopathologic diagnosis was consistent with pyoderma gangrenosum.
A 70-year-old man presented with persistent cough productive of clear sputum which had persisted approximately 12 months after COVID-19 infection. The patient reported a more recent history of night sweats and had also recently developed what he described as “blisters” on his chest wall and right shoulder starting 4 weeks prior to presentation that “opened up” giving off a bloody discharge. The patient had been treated with trimethoprim-sulfamethoxazole and doxycycline without improvement and reported a 10-pound weight loss over the past several months. The patient was a never-smoker with no significant travel history and a past medical history of asthma, GERD, gout, and chronic rhinitis. He had no history of autoimmune/inflammatory diseases or malignancy.
Vital signs and physical exam were normal, except for a 1 cm open wound in the center of the patient’s chest [Figure 2A]. A chest CT performed as part of the patient’s workup demonstrated a spiculated mass in the left upper lobe with adjacent mediastinal adenopathy [Figure 1A-C]. This prompted an FDG PET-CT, which demonstrated some increased uptake in the mass and adjacent lymph nodes [Figure 1D]. The mass was biopsied via bronchoscopy, pathology was nondiagnostic with rare groups of benign-appearing bronchial epithelial cells and blood. The skin lesion was biopsied next demonstrating dense mixed neutrophilic dermal inflammation [Figure 2B]. The diagnosis of pyoderma gangrenosum was made and the patient was treated with NSAIDs and a systemic glucocorticoid (40 mg/day, tapered over 10 weeks).steroid taper, The pulmonary mass , mediastinal lymph nodes and skin lesions all resolved over time.
Pyoderma gangrenous (PG) is a misnomer in every sense as it is neither infectious nor gangrenous. It is a rare (3-10 cases/million/year) disorder of skin characterized by neutrophilic dermatosis which usually presents as a with inflammatory and ulcerative disorder of the skin lesions and is usually a diagnosis of exclusion (1). PG has no pathognomonic clinical or histological findings. Majority of the cases have an underlying systemic disease, commonly inflammatory bowel disease (41%), inflammatory arthritis (20.5%) and oncologic or hematologic disorders (17.2%). While it can in any age group including children, the peak age of onset is 40-60 years. There is a slight female preponderance (2). The most common presentation is inflammatory papule or pustule that progress to a painful ulcer with violaceous undermined borders and a purulent base. The lesions commonly occur in surgical wounds within 2 weeks of surgery, a phenomenon known as pathergy, and often lead to wound dehiscence (3). The lesions may also be peristomal in patients with IBD. Extracutaneous lesions have been reported in liver, intestine, spleen, cornea, bones, muscles, CNS and rarely, in the lungs (4-6).
There have been <50 cases of pulmonary PG ever described in literature (7,8). The patients may present with non-specific symptoms of cough, dyspnea, fever, weight-loss, malaise and occasionally hemoptysis. Chest imaging may show cavitary infiltrates. The diagnosis is established by cutaneous or extracutaneous lesion biopsy of the ulcer edge showing neutrophilic infiltrate. Extensive testing should be performed , extensive testing to rule out alternative causes including infection, and malignancy, in setting of underlying inflammatory bowel disease or inflammatory arthritisautoimmune and inflammatory conditions associated with PG. Presence of pathergy and response to anti-inflammatory therapy also support the diagnosis (9). Treatment includes systemic or intralesional glucocorticoids and/or calcineurin inhibitors (3). Use of TNF alpha inhibitor, infliximab and anti-neutrophil antimicrobial dapsone has also been described in case reports (10). Most patients achieve remission within 6 months to 3 years.
Umesh Goswami MD1, Michael Gotway MD2, Carlos Rojas MD2, Prasad Panse MD2, Kris Cummings MD2, Eric Jensen MD2, Kenneth Sakata, MD1 and Clinton Jokerst MD2
Division of Pulmonology1 and Department of Radiology2
Mayo Clinic Arizona, Scottsdale, AZ USA
References
- Ruocco E, Sangiuliano S, Gravina AG, Miranda A, Nicoletti G. Pyoderma gangrenosum: an updated review. J Eur Acad Dermatol Venereol. 2009 Sep;23(9):1008-17. [CrossRef] [PubMed]
- Ashchyan HJ, Butler DC, Nelson CA, et al. The Association of Age With Clinical Presentation and Comorbidities of Pyoderma Gangrenosum. JAMA Dermatol. 2018 Apr 1;154(4):409-413. [CrossRef] [PubMed]
- Binus AM, Qureshi AA, Li VW, Winterfield LS. Pyoderma gangrenosum: a retrospective review of patient characteristics, comorbidities and therapy in 103 patients. Br J Dermatol. 2011 Dec;165(6):1244-50. [CrossRef] [PubMed]
- Vadillo M, Jucgla A, Podzamczer D, Rufi G, Domingo A. Pyoderma gangrenosum with liver, spleen and bone involvement in a patient with chronic myelomonocytic leukaemia. Br J Dermatol. 1999 Sep;141(3):541-3. [CrossRef] [PubMed]
- Scherlinger M, Guillet S, Doutre MS, Beylot-Barry M, Pham-Ledard A. Pyoderma gangrenosum with extensive pulmonary involvement. J Eur Acad Dermatol Venereol. 2017 Apr;31(4):e214-e216. [CrossRef] [PubMed]
- Abdelrazeq AS, Lund JN, Leveson SH. Pouchitis-associated pyoderma gangrenosum following restorative proctocolectomy for ulcerative colitis. Eur J Gastroenterol Hepatol. 2004 Oct;16(10):1057-8. [CrossRef] [PubMed]
- Gade M, Studstrup F, Andersen AK, Hilberg O, Fogh C, Bendstrup E. Pulmonary manifestations of pyoderma gangrenosum: 2 cases and a review of the literature. Respir Med. 2015 Apr;109(4):443-50. [CrossRef] [PubMed]
- Sakata KK, Penupolu S, Colby TV, Gotway MB, Wesselius LJ. Pulmonary pyoderma gangrenosum without cutaneous manifestations. Clin Respir J. 2016 Jul;10(4):508-11. [CrossRef] [PubMed]
- Maverakis E, Ma C, Shinkai K, et al. Diagnostic Criteria of Ulcerative Pyoderma Gangrenosum: A Delphi Consensus of International Experts. JAMA Dermatol. 2018 Apr 1;154(4):461-466. [CrossRef] [PubMed]
- Teasley LA, Foster CS, Baltatzis S. Sclerokeratitis and facial skin lesions: a case report of pyoderma gangrenosum and its response to dapsone therapy. Cornea. 2007 Feb;26(2):215-9. [CrossRef] [PubMed]
Cite as: Goswami U, Gotway M, Rojas C, Panse P, Cummings K, Jensen E, Sakata K, Jokerst C. July 2022 Medical Image of the Month: Pulmonary Nodule in the Setting of Pyoderma Gangrenosum (PG). Southwest J Pulm Crit Care Sleep. 2022:25(1):4-6. doi: https://doi.org/10.13175/swjpccs029-22 PDF
June 2022 Medical Image of the Month: A Hard Image to Swallow
Alessandra Carrillo, DO
Robert Ondracek, DO
Shil Punatar, DO
Andrew Ondracek, DO
Ravi Sundaram, DO
Department of Critical Care Medicine
Franciscan Health
Olympia Fields, Illinois USA

Figure 1. Portable chest x-ray demonstrating marked dilatation of the esophagus with food impaction and bilateral aspiration of food particles. There is also a small left pleural effusion.

Figure 2. Coronal view CT-chest/abdomen/pelvis demonstrating marked dilatation of the esophagus with food impaction seen and food particles seen in his lungs bilaterally.
Introduction
Esophageal food impactions are common occurrences in gastroenterology, however, under 20% of cases require intervention (1) .The clinical condition of the esophagus and the consistency of food being swallowed contribute to the development of food bolus impactions, with patients having underlying esophageal pathology in most cases (2). Unfortunately, radiographic evidence is often difficult to obtain as food is radiolucent and poorly visualized on radiograph. Here, we demonstrate the risk associated with severe food impaction.
Case Presentation
An 86-year-old man with a past medical history of achalasia with laparoscopic Heller myotomy complicated by distal esophageal perforation, was admitted after presenting with complaints of chest pain and inability to tolerate a solid diet. Additionally, he suffered a 90-pound weight loss over 1 year. He was seen by speech therapy and provided with a dysphagia appropriate diet. Eight days into the patient stay, the family presented to the patient's bedside to assist in 1-to-1 feeding of the patient per their request. One hour following the completion of the patient’s feeding, a CODE BLUE was called. The patient was unresponsive and without a pulse. PEA protocol was initiated and return of spontaneous circulation was achieved. Post intubation chest x-ray demonstrated a markedly dilated esophagus (Figures 1). Thereafter, CT chest was ordered demonstrating markedly dilated appearance of the patient’s esophagus with internal food material without as a large obstructing lesion (Figure 2). This was deemed to be the cause of the patient's cardiac arrest with concomitant aspiration. Overall, the dilatation significantly progressed from previous imaging. The patient was made NPO, transitioned to total parenteral nutrition and plans were made for a follow-up disimpaction via esophagogastroduodenoscopy (EGD). Ultimately, the patient was too unstable to pursue EGD and expired 9 days after his initial arrest.
Discussion
Through literature review, a majority of cases of food bolus impaction are self-limited. In most cases described, boluses pass on their own or with the assistance of an EGD. In most cases, underlying esophageal or motility dysfunction is known. With few case reports, food disimpaction has been assisted with cola products or nifedipine (3,4). Though trivially regarded, our case demonstrates that food bolus revel against more gruesome esophageal pathology in both presentation, prompt intervention, and adverse on outcomes.
Conclusions
We illustrate a common presentation to gastroenterologists and physicians of a food bolus impaction. Though, due to the profound radiographic presentation and severe morbidity of our clinical scenario, we hope to bring attention to the need for rapid evaluation, treatment, and consideration of adverse outcomes in patients presenting with food boluses as well as the severity and life-threatening outcomes that may preside with the previously trivially described pathology.
References
- Yao CC, Wu IT, Lu LS, Lin SC, Liang CM, Kuo YH, Yang SC, Wu CK, Wang HM, Kuo CH, Chiou SS, Wu KL, Chiu YC, Chuah SK, Tai WC. Endoscopic Management of Foreign Bodies in the Upper Gastrointestinal Tract of Adults. Biomed Res Int. 2015;2015:658602. [CrossRef] [PubMed]
- Sperry SL, Crockett SD, Miller CB, Shaheen NJ, Dellon ES. Esophageal foreign-body impactions: epidemiology, time trends, and the impact of the increasing prevalence of eosinophilic esophagitis. Gastrointest Endosc. 2011 Nov;74(5):985-91. [CrossRef] [PubMed]
- Gelfond M, Rozen P, Gilat T. Isosorbide dinitrate and nifedipine treatment of achalasia: a clinical, manometric and radionuclide evaluation. Gastroenterology. 1982 Nov;83(5):963-9. [PubMed]
- Karanjia ND, Rees M. The use of Coca-Cola in the management of bolus obstruction in benign oesophageal stricture. Ann R Coll Surg Engl. 1993 Mar;75(2):94-5. [PubMed]
May 2022 Imaging Case of the Month: Asymmetric Apical Opacity–Diagnostic Considerations
Department of Radiology
Mayo Clinic, Arizona
Phoenix, Arizona USA
Clinical History: A 64–year–old woman presented to the emergency room with complaints of right arm pain for 2 months accompanied by subjective low-grade intermittent fevers.
The patient’s past medical history was unremarkable and she had never had surgery. She had been a smoker for most of her life, at least 25-pack-years. She denied allergies, admitted to moderate daily alcohol use, and denied illicit drug use.
The patient’s physical examination showed no clear focal abnormalities and she was afebrile. She did have some right scapular tenderness to palpation, although there were no abnormal skin changes over this region. Her pulse rate and blood pressure were within normal limits, and her room air oxygen saturation was 96%. Basic laboratory data, including a complete blood count and electrolytes were largely within the normal range. The patient’s white blood cell count was technically abnormal at 9.7 x109 (normal, 3.4 - 9.6 x 109), but there was no left shift and the treating emergency room physician felt the mildly elevated white blood cell count was of no clinical significance.
Frontal and lateral chest radiography (Figure 1) was performed.

Figure 1. Frontal (A) and lateral (B) chest radiography.
Which of the following represents an appropriate interpretation of her frontal chest and lateral radiograph? (Click on the correct answer to be directed to the second of twelve pages)
- Frontal chest radiography shows multifocal consolidation
- Frontal chest radiograph shows numerous small nodules
- Frontal chest radiography shows a focal mass
- Frontal chest radiography shows a destructive bone lesion
- Frontal chest radiography shows pleural effusion
March 2022 Medical Image of the Month: Pulmonary Nodules in the Setting of Diffuse Idiopathic Pulmonary NeuroEndocrine Cell Hyperplasia (DIPNECH)

Figure 1. Unenhanced chest CT images in the axial plane show solid, non-calcified and well-circumscribed nodules in the right upper lobe (RUL) (A) and lingula (B). The RUL nodule is FDG-avid on axial fused FDG PET-CT image (C) whereas the lingular nodule is not (D).

Figure 2. Unenhanced chest CT images in the axial plane reconstructed with maximum intensity projection (MIP, A) and minimum intensity projection (MinIP, B) techniques show multiple scattered solid pulmonary nodules (arrows) and pulmonary mosaicism consistent with air-trapping (circled). Axial fused images from a 68GA-DOTATATE PET-CT demonstrate some activity in the RUL nodule (C) and more prominent uptake in the lingular nodule (D).

Figure 3. Hematoxylin and Eosin stained low-power pathological image (A) demonstrates the lingular carcinoid tumor (*) as well as several carcinoid tumorlets (arrows) in the adjacent lung. A separate specimen of lung stained with synaptophysin demonstrates multiple tumorlets in the small sample. When taken in conjunction with imaging findings, pathology is in-keeping with a diagnosis of Diffuse Idiopathic Pulmonary Neuroendocrine Cell Hyperplasia (DIPNECH).
A 62-year-old woman presented to an outside hospital with chronic cough, prompting a chest x-ray (CXR). Findings further prompted unenhanced chest CT to evaluate possible pulmonary nodules. The CT demonstrated multiple scattered, solid and centrilobular pulmonary nodules, most of which were small but there were two >1 cm nodules, one in the right upper lobe (RUL) and a second in the lingula (Figure 1A,B). A subsequent FDG PET-CT was performed demonstrating increased metabolic activity in the RUL nodule with no activity in the lingular nodule (Figure 1C,D). Biopsy of the RUL nodule was consistent with a carcinoid. At this point the patient was referred to our center for further management. A repeat chest CT failed to demonstrate any significant change in the nodules. MIP and MinIP reconstructions from that examination demonstrate multiple small, solid pulmonary nodules (arrows) (Figure 2A), many of which were associated with air-trapping resulting in pulmonary mosaicism (circled) (Figure 2B). A 68GA-DOTATATE PET-CT was performed, the results of which provide stark contrast to the FDG-PET in that the RUL nodule demonstrated modest uptake (Figure 2C), whereas the lingular nodule showed very prominent update (Figure 2D). The lingular nodule was resected, H & E-stained pathology image (Figure 3A) demonstrated a typical carcinoid (*) with multiple carcinoid tumorlets in the surgical specimen (arrows). A separate specimen stained with synaptophysin demonstrates multiple neuroendocrine tumorlets. Pathological findings, in conjunction with patient demographics and imaging findings, were consistent with Diffuse Idiopathic Pulmonary NeuroEndocrine Cell Hyperplasia (DIPNECH).
DIPNECH is recognized as a pre-neoplastic lesion in the 2015 WHO classification of lung tumors (1). There is neuroendocrine cell proliferation within the small bronchi and bronchioles which may progress beyond the basement membrane, forming carcinoid tumorlets and in some cases, eventually carcinoid tumors. These airway-centered nodules cause obstruction. In addition, there is often an association between DIPNECH and constrictive bronchiolitis, which causes further airway obstruction (2). The vast majority of patients are women in their 50s-70s and most patients are symptomatic with the most common presenting symptoms being chronic cough and dyspnea (3,4). Many of these patients are often mis-diagnosed with asthma initially (4). The imaging findings of DIPNECH on CT are not specific but can be pathognomonic in some cases. There are almost always innumerable small solid (and sometimes ground glass) centrilobular nodules and nodular bronchial thickening with associated pulmonary mosaicism related to air trapping. Nodules are either stable or very slowly growing over years with the largest nodules usually being biopsied or resected and yielding typical carcinoid on pathology (4). A relatively new nuclear medicine imaging study, 68Ga-DOTATATE PET-CT, shows promise as a higher resolution and more sensitive examination for detection of neuroendocrine tumors (relative to octreotide scans), including pulmonary carcinoid tumors in the setting of DIPNECH (5,6).
Clinton Jokerst MD1, Henry Tazelaar2, Carlos Rojas MD1, Prasad Panse MD1, Kris Cummings MD1, Eric Jensen MD1 and Michael Gotway MD1
Departments of Radiology1 and Pathology2
Mayo Clinic Arizona, Scottsdale, AZ USA
References
- Gosney JR, Austin JHM, Jett J, et al. Diffuse pulmonary neuroendocrine cell hyperplasia. In: Travis WD, Brambilla E, Burke AP, et al., eds. WHO classification of tumours of the lung, pleura, thymus and heart. Lyon, IARC Press, 2015; pp. 78-79.
- Samhouri BF, Azadeh N, Halfdanarson TR, Yi ES, Ryu JH. Constrictive bronchiolitis in diffuse idiopathic pulmonary neuroendocrine cell hyperplasia. ERJ Open Res. 2020 Nov 16;6(4):00527-2020. [CrossRef] [PubMed]
- Rossi G, Cavazza A, Spagnolo P, Sverzellati N, Longo L, Jukna A, Montanari G, Carbonelli C, Vincenzi G, Bogina G, Franco R, Tiseo M, Cottin V, Colby TV. Diffuse idiopathic pulmonary neuroendocrine cell hyperplasia syndrome. Eur Respir J. 2016 Jun;47(6):1829-41. [CrossRef] [PubMed]
- Little BP, Junn JC, Zheng KS, Sanchez FW, Henry TS, Veeraraghavan S, Berkowitz EA. Diffuse Idiopathic Pulmonary Neuroendocrine Cell Hyperplasia: Imaging and Clinical Features of a Frequently Delayed Diagnosis. AJR Am J Roentgenol. 2020 Dec;215(6):1312-1320. [CrossRef] [PubMed]
- Deppen SA, Blume J, Bobbey AJ, Shah C, Graham MM, Lee P, Delbeke D, Walker RC. 68Ga-DOTATATE Compared with 111In-DTPA-Octreotide and Conventional Imaging for Pulmonary and Gastroenteropancreatic Neuroendocrine Tumors: A Systematic Review and Meta-Analysis. J Nucl Med. 2016 Jun;57(6):872-8. [CrossRef] [PubMed]
- Fraum TJ, Ritter JH, Chen DL. Diffuse Idiopathic Pulmonary Neuroendocrine Cell Hyperplasia on Somatostatin Receptor Imaging. Am J Respir Crit Care Med. 2018 Nov 1;198(9):1223-1225. [CrossRef] [PubMed]
Cite as: Jokerst C, Tazelaar H, Rojas C, Panse P, Cummings K, Jensen E, Gotway M. March 2022 Medical Image of the Month: Pulmonary Nodules in the Setting of Diffuse Idiopathic Pulmonary Neuroendocrine Cell Hyperplasia (DIPNECH). Southwest J Pulm Crit Care Sleep;2022:40-42. doi: https://doi.org/10.13175/swjpccs010-22 PDF
February 2022 Medical Image of the Month: Multifocal Micronodular Pneumocyte Hyperplasia in the Setting of Tuberous Sclerosis

Figure 1. Unenhanced chest CT in the axial (A) plane showing multiple subsolid pulmonary nodules in a random distribution (arrows). Unenhanced chest CT in the axial (A) plane compared to an image from a contrast-enhanced abdominal CT performed 1 year earlier (B) shows relative stability of these nodules (arrows). In a 22 y/o man with known Tuberous Sclerosis Complex, these findings are consistent with Multifocal Micronodular Pneumocyte Hyperplasia. Click here to view Figure 1 in an enlarged window.
{kind=link}

Figure 2. Unenhanced chest CT in the axial (A) plane, soft tissue window display settings, demonstrate foci of myocardial fat (arrow). Unenhanced chest CT in the axial (B) and sagittal (C) planes, bone window display settings, shows multiple small scattered sclerotic osseous foci (circles). These ancillary findings are quite common in the setting of tuberous sclerosis. Click here to view Figure 2 in an enlarged window.
{kind=link}
A 22-year-old man with a known diagnosis of Tuberous Sclerosis Complex (TSC) presents for a follow-up unenhanced chest CT to re-evaluate pulmonary nodules seen in the lung bases on a prior abdominal CT. The patient also has a history of multiple renal lesions consistent with lipid-poor angiomyolipomas based on previous abdominal MRI findings. The chest CT demonstrated multiple scattered, randomly distributed sub-centimeter pulmonary nodules of solid or subsolid morphology [Figure 1A]. Those nodules visible in the lung bases on the prior abdominal CT had remined stable over the 12-month interval consistent with multifocal microscopic pneumocyte hyperplasia (MMPH)[Figure 1B,C]. Myocardial fatty foci (MFF) were visualized in the heart on soft tissue window display settings [Figure 2A] as were multiple scattered sclerotic bone lesions on bone window display settings [Figure 2B,C]. No pulmonary cysts were seen to suggest lymphangioleiomyomatosis (LAM) and there were no thoracic lymphangiomas.
MMPH represents a benign hamartomatous proliferation of type II pneumocytes which manifest as small, randomly scattered pulmonary nodules that can be solid or subsolid and are self-limited (1). MMPH is rare in general, but quite common in TSC with a reported incidence as high as 71% (2). MMPH does not demonstrate a sex predilection (unlike LAM in TSC). It is important to remember MMPH in the setting of TSC as it represents a “don’t touch” lesion; recognizing it as such can save unnecessary trouble for the patient (3). The MFF seen on this chest CT also is a relatively common and specific finding in TSC, seen in at least 50% of TSC patients (4,5). Although MMPH and MFF appear to be relatively specific imaging findings in the setting of TSC, as of yet they have not been incorporated into the diagnostic criteria for TSC (6). The small sclerotic bone lesions, especially involving the posterior elements of the spine, are also a well described finding in TSC; however, this finding is much less specific and can be seen in many conditions (7).
Clinton Jokerst MD, Carlos Rojas MD, Prasad Panse MD, Kris Cummings MD, Eric Jensen MD and Michael Gotway MD
Department of Radiology
Mayo Clinic Arizona
Scottsdale, AZ USA
References
- Franz DN, Brody A, Meyer C, Leonard J, Chuck G, Dabora S, Sethuraman G, Colby TV, Kwiatkowski DJ, McCormack FX. Mutational and radiographic analysis of pulmonary disease consistent with lymphangioleiomyomatosis and micronodular pneumocyte hyperplasia in women with tuberous sclerosis. Am J Respir Crit Care Med. 2001 Aug 15;164(4):661-8. [CrossRef] [PubMed]
- Wataya-Kaneda M, Tanaka M, Hamasaki T, Katayama I. Trends in the prevalence of tuberous sclerosis complex manifestations: an epidemiological study of 166 Japanese patients. PLoS One. 2013 May 17;8(5):e63910. [CrossRef] [PubMed]
- Aswani Y, Gavai B. Multifocal micronodular pneumocyte hyperplasia: A "touch-me-not" pulmonary lesion in tuberous sclerosis complex. Lung India. 2018 Sep-Oct;35(5):445-446. [CrossRef] [PubMed]
- Adriaensen ME, Schaefer-Prokop CM, Duyndam DA, Zonnenberg BA, Prokop M. Fatty foci in the myocardium in patients with tuberous sclerosis complex: common finding at CT. Radiology. 2009 Nov;253(2):359-63. [CrossRef] [PubMed]
- Tresoldi S, Munari A, Di Leo G, Pompili G, Magistrelli P, Secchi F, La Briola F, Canevini MP, Cornalba G, Sardanelli F. Myocardial Fatty Foci in Adult Patients with Tuberous Sclerosis Complex: Association with Gene Mutation and Multiorgan Involvement. Radiology. 2015 Nov;277(2):398-405. [CrossRef] [PubMed]
- Northrup H, Krueger DA; International Tuberous Sclerosis Complex Consensus Group. Tuberous sclerosis complex diagnostic criteria update: recommendations of the 2012 Iinternational Tuberous Sclerosis Complex Consensus Conference. Pediatr Neurol. 2013 Oct;49(4):243-54. [CrossRef] [PubMed]
- Baskin HJ Jr. The pathogenesis and imaging of the tuberous sclerosis complex. Pediatr Radiol. 2008 Sep;38(9):936-52. [CrossRef] [PubMed]
February 2022 Imaging Case of the Month: Between A Rock and a Hard Place
Department of Radiology, Mayo Clinic, Arizona
5777 East Mayo Boulevard
Phoenix, Arizona USA
Clinical History: A 46-year-old woman presented to her primary care physician with longstanding complaints of difficulty with aerobic exercise, near syncope, headache, poor sleep, and pain in both legs and arms, exacerbated when flying in commercial aircraft. The patient had also complained of several gastrointestinal disturbances recently that prompted evaluation, revealing a normal colonoscopy. The patient was diagnosed with probable food intolerance by breath testing showing fructose intolerance, managed with a low fermentable oligosaccharides, disaccharides, monosaccharides and polyols (FODMAP) diet with positive results.
PMH, SH, FH: The patient’s past medical history was remarkable for a history of Raynaud’s phenomenon and head trauma at age 16. She noted that her presenting complaints have been present since childhood to some extent. Her poor sleep was characterized as frequent awakenings, daytime somnolence, mouth dryness, and waking up with severe headaches. The patient had been diagnosed with COVID-19 4 months earlier, with her presenting complaints all exacerbated and accompanied by shortness of breath, but she recovered uneventfully. The patient denied other significant past medical history and had no surgical history. Her family history was remarkable for a sister diagnosed with obstructive sleep apnea, diabetes, and thyroid carcinoma, and hypertension in a number of her 13 siblings. The patient’s mother had been diagnosed with colonic malignancy and her father died of melanoma. The patient’s social history was remarkable for abuse during childhood by a male sibling. The patient denied tobacco, alcohol, and illicit drug use.
Physical Examination: The patient’s physical examination showed her to be slender and in no distress although anxious, afebrile, pulse rate= 73, normal respiratory rate, with a blood pressure of 116/95 mmHg. Her cardiovascular, pulmonary, musculoskeletal, and neurologic examinations were within normal limits.
Results from prior outside examinations, including funduscopic, abdominal MRI, and brain MRI and MRA were within normal limits. An outside audiology consultation when the patient complained of hearing loss several months after her SARS-CoV-2 infection showed normal findings. Her complete blood count, coagulation parameters, electrolytes, and liver panel showed no abnormal values. A frontal chest radiograph from an outside institution (Figure 1) from 4 months prior to her primary care appointment, around the time when the patient was diagnosed with COVID-19.
 P
P

Figure 1. Frontal (A) and lateral (B) chest radiography obtained around the time the patient was diagnosed with COVID-19.
Which of the following represents an appropriate interpretation of her frontal chest radiograph? (Click on the correct answer to be directed to the second of 11 pages)
- Frontal chest radiography shows findings typical for coronavirus (SARS-CoV-2) pulmonary infection
- Frontal chest radiograph shows bilateral peribronchial lymphadenopathy
- Frontal chest radiography shows focal consolidation
- Frontal chest radiography shows multiple lung nodules
- Frontal chest radiography shows pleural effusion
Cite as: Gotway MB. February 2022 Imaging Case of the Month: Between A Rock in a Hard Place. Southwest J Pulm Crit Care Sleep. 2022;24(2): 12- . doi: https://doi.org/10.13175/swjpccs004-22 PDF
January 2022 Medical Image of the Month: Bronchial Obstruction Due to Pledget in Airway Following Foregut Cyst Resection

Figure 1. Enhanced chest CT in axial (A), sagittal (B), and coronal (C) planes shows a mediastinal foregut duplication cyst (*) compressing medial basal subsegmental airways (arrows). Axial enhanced chest CT displayed in lung (A and B) and soft tissue (C) windows 7 years after surgical resection of the foregut duplication cyst shows post-resection changes with a focus of hyperattenuation (curved arrow) related to the medial basal segmental bronchus; this bronchus is dilated and fluid-filled more distally (arrow). Click here to view Figure 1 enlarged in a new window.
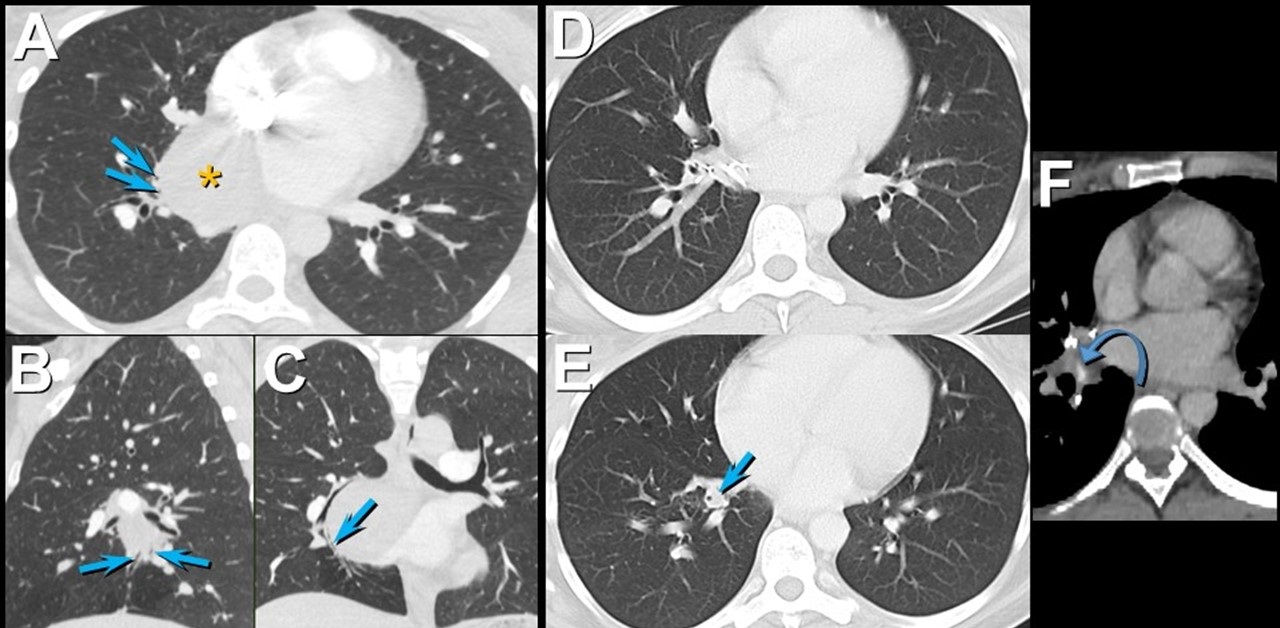{kind=link}

Figure 2. Bronchoscopic images (G-J) show an object obstructing the medial basal segmental right lower lobe bronchus (arrow); a blue suture is attached to the object. The object (arrow) was retrieved using forceps (arrowhead) and was found to reflect a surgical pledget. Follow up unenhanced axial (K), sagittal (L), and coronal (M) chest CT shows mildly stenosed medial basal subsegmental bronchi (curved arrow) with distal bronchiectasis (double arrowheads); these airway abnormalities are shown to advantage using minimum intensity projected images (N-P). Click here to view Figure 2 enlarged in a new window.
{kind=link}
A 37-year-old woman complaining of chest pain and cough underwent resection of a mediastinal foregut duplication cyst complicated by a 10-day hospitalization with a prolonged air leak. Seven years later, she presented with worsening cough and shortness of breath, complaining of similar symptoms intermittently in the 7 years between her surgery and presentation. Chest CT showed a hyperattenuating lesion obstructing the medial basal segmental airways (Figure 1). Bronchoscopy revealed a suture and a pledget obstructing the medial basal segmental right lower lobe bronchus (Figure 2). The pledget and suture were successfully removed. Repeat bronchoscopy several months later showed no residual airway foreign body, although medial basal subsegmental bronchial stenosis prevented advancement of the bronchoscope distally; this finding correlated with the CT impression of airway stenosis or occlusion in this region on the follow up CT.
Bronchogenic cysts result from abnormal lung budding and development of the ventral foregut during the first trimester (1). Many lesions are detected asymptomatically, but larger lesions, as in this patient, may induce symptoms prompting resection. The surgical note for this patient suggested the lesion resided in the right lower lobe, but most bronchogenic cysts arise in the mediastinum near the carina, and this patient’s large lesion extended from the subcarinal space into the azygoesophageal recess. It is possible the surgeon entered the right lower lobe to resect the lesion, resulting in the post-surgical air as well as the surgical pledgets in the medial basal right lower lobe airway that caused the patient’s recurrent chest complaints.
Prasad M. Panse MD1 and Kenneth K. Sakata MD2
Departments of Radiology1 and Pulmonary Medicine2
Mayo Clinic Arizona, Scottsdale, AZ USA
Reference
- Panchanatheeswaran K, Dutta R, Singh KI, Kumar A. Eleven-year experience in thoracoscopic excision of bronchogenic cyst. Asian Cardiovasc Thorac Ann. 2012; 20(5):570-574 perspective. Natl J Maxillofac Surg. 2015; 6(2):144-1451. [CrossRef][PubMed]
Cite as: Panse PM, Sakata KK. January 2022 medical image of the month: bronchial obstruction due to pledget in airway following foregut cyst resection. Southwest J Pulm Crit Care. 2022;24(1):6-7. doi: https://doi.org/10.13175/swjpcc065-21 PDF
December 2021 Medical Image of the Month: Aspirated Dental Implant

Figure 1. Frontal and lateral chest radiography shows right middle and lower lobe consolidation and a large right pleural effusion, suggesting pneumonia and parapneumonic effusion, but also shows a metallic focus in the right lower lobe. Click here to view Figure 1 enlarged in a new window.
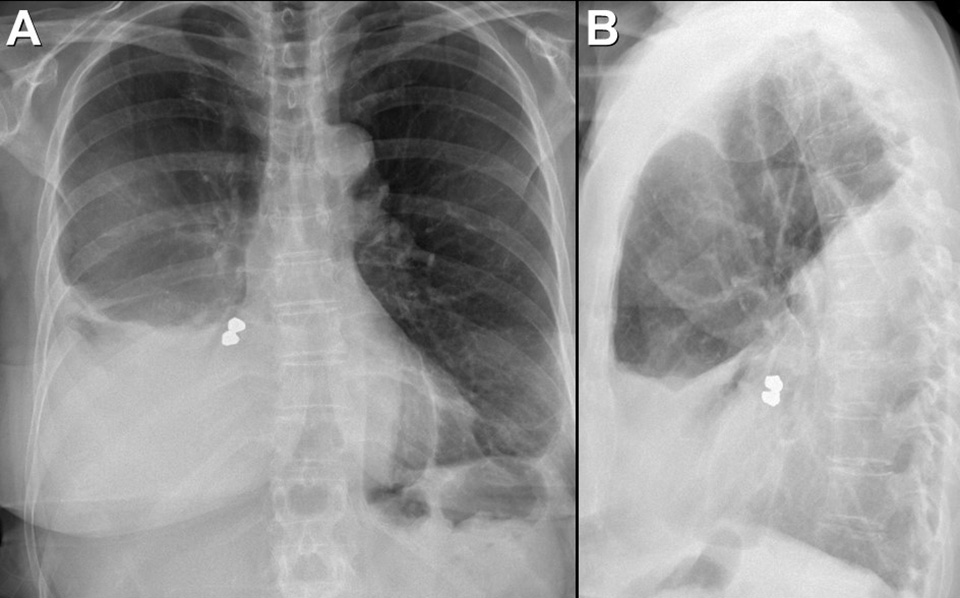{kind=link}

Figure 2. Axial (A and B), sagittal (C) and coronal (D) contrast-enhanced chest CT displayed in soft tissue (A) and bone (B-D) windows shows right lower lobe consolidation and loculated pleural effusion. A metallic focus closely related to the right lower lobe bronchus is present. Click here to view Figure 2 enlarged in a new window.
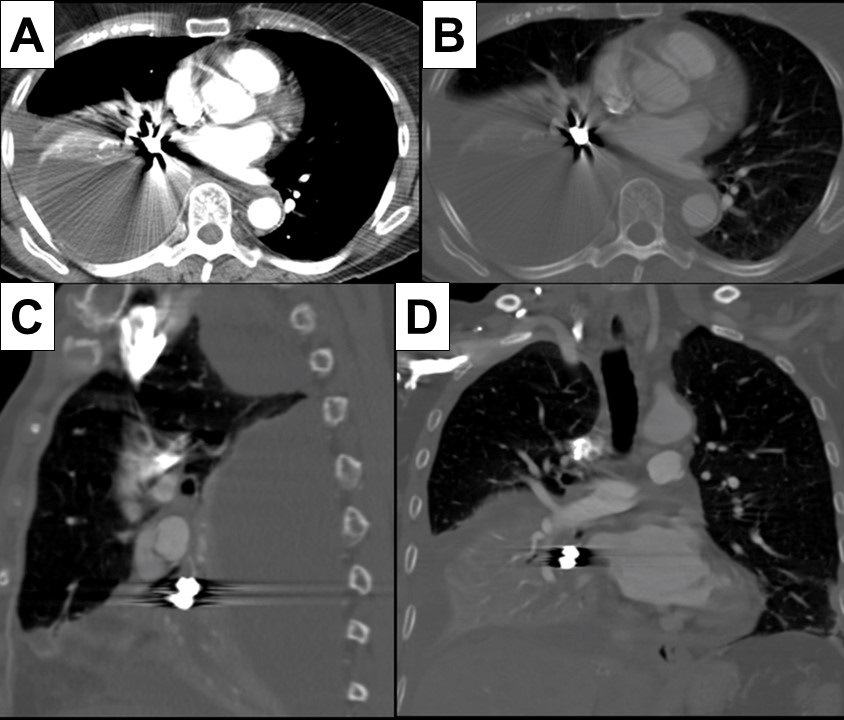{kind=link}

Figure 3. Bronchoscopic images performed during retrieval of the right lower lobe foreign body shows a metallic object lodged within the right lower lobe bronchus. The object was retrieved using a forceps and found to represent a dental implant, evidently aspirated during the patient’s prolonged dental procedure. Click here to view Figure 3 enlarged in a new window.
{kind=link}
A 76-year-old woman with a past medical history significant for left-sided breast cancer status post lumpectomy recently underwent an extensive dental procedure about 1 month prior to presentation. The dental procedure was prolonged, and the patient reported falling asleep during the procedure several times. She presented with fatigue, right pleuritic chest pain, low-grade fevers, and drenching sweats. She underwent chest radiography at an outside institution which disclosed pneumonia, for which she was treated with cefdinir and doxycycline without improvement. Thoracostomy tube drainage of the pleural effusion was performed and showed empyema. Imaging showed an airway foreign body which was retrieved bronchoscopically. The patient made an uneventful recovery.
Aspiration during dental procedures is rare but reported (1). Dental items have been reported as the second most commonly ingested/aspirated foreign objects in adults. If the airway is not compromised, assessment for any lost or missing instrument and its component should be done promptly with a high suspicion of mishap. Fortunately, many dental appliances and instruments are often, but not always, radiopaque and may be detected by chest radiography. Many can be removed by bronchoscopy, as in this case.
Prasad M. Panse MD1, Sreeja Biswas Roy MD2, Robert W. Viggiano MD2
Departments of Radiology1 and Pulmonary Medicine2
Mayo Clinic Arizona
Scottsdale, AZ USA
Reference
- Yadav RK, Yadav HK, Chandra A, Yadav S, Verma P, Shakya VK. Accidental aspiration/ingestion of foreign bodies in dentistry: A clinical and legal perspective. Natl J Maxillofac Surg. 2015; 6(2):144-1451. [CrossRef] [PubMed]
Cite as: Panse PM, Biswas Roy S, Viggiano RW. December 2021 Medical Image of the Month: Aspirated Dental Implant. Southwest J Pulm Crit Care. 2021;23(6):149-50. doi: https://doi.org/10.13175/swjpcc040-21 PDF
Medical Image of the Month: Cavitating Pseudomonas aeruginosa Pneumonia

Figure 1. A: Admission CXR demonstrates upper lobe bullae and left peri-hilar consolidation on background of emphysema. B: Day 4 CXR reveals more confluent consolidation and opacification of the bullous change. C: Day 8 CXR demonstrates air fluid level with increasing density of consolidation. D: Repeat CXR 6 weeks after discharge shows near complete resolution of findings with small residual cavity.

Figure 2. CT Chest with contrast confirmed extensive consolidation with cavitation and suggested possibility of atypical infection
Case Presentation
A 56-year-old woman presented with cough and shortness of breath to hospital. She had a temperature of 39.2°C and had recently completed course of steroids and antibiotics for exacerbation of chronic obstructive pulmonary disease (COPD). She was an active smoker of 15 cigarettes/day for about 40 years. No other past medical history was noted. On examination she had left-sided crepitations and oxygen saturations of 90% on room air.
Chest x-ray (CXR) (Fig 1:A) showed features of background emphysema with upper lobe peripheral bullae, larger on the left. Dense left peri-hilar consolidation was also described. SARS-CoV-2 swab was negative. White blood cells (WBC) were raised at 16.9x109/L and C-reactive protein (CRP) at 331 mg/L. The rest of the blood tests were unremarkable. CURB-65 score was zero but treatment was commenced with intravenous (IV) amoxicillin & oral clarithromycin in view of level of CRP and CXR findings. On Day 4 of admission CRP spiked to 541 mg/L. Repeat CXR (Fig 1:B) showed more confluent left upper zone consolidation and increased opacification of bullous change in the left apex. Microbiologist advised switch of IV Amoxicillin to IV Co-amoxiclav. Respiratory colleagues suggested to check sputum for acid-fast bacilli (AFB). Pneumococcal & legionella urinary antigens came back negative. HIV was also excluded. Growth of Pseudomonas aeruginosa was detected on a blood-tinged sputum sample which was confirmed on 3 more subsequent samples. AFB stain was persistently negative. Blood cultures did not yield any growth.
Antibiotic therapy was escalated to IV piperacillin/tazobactam (Tazocin; Pfizer; UK) QDS (Pseudomonas dose) in light of the new finding. Inflammatory markers slowly started to shift but intermittent temperature spikes continued so repeat CXR (Fig 1:C) and subsequent computed tomography (CT) of chest with contrast (Fig 2) were obtained to assess the complex pneumonia with its striking appearances. CT confirmed extensive consolidation with cavitation and air-fluid levels in the left apical region. Patient required 2L/min supplemental oxygen at the time. By completion of 7-day course of IV piperacillin/tazobactam CRP dropped to 63 mg/L and WBC to 8.6x109/L. Patient was successfully weaned off oxygen and discharged home. Repeat CXR in 6 weeks (Fig 1:D) showed marked improvement with residual small cavity.
Discussion
P. Aeruginosa - a gram negative rod is a rare cause of both CAP (community acquired pneumonia) and cavitating pneumonia. It is more commonly associated with hospital acquired pneumonia (HAP) and usually affects immunocompromised hosts (1). Cavitating pneumonia arises as a result of necrosis of lung parenchyma due to toxins derived from bacterial pathogens. Maharaj et al. (2) reviewed 9 cases of P. Aeruginosa CAP reported on PubMed from 2001 to 2016 and 5 out of 9 patients were found to be smokers. Emphysema was reported in 2 and asthma only in 1 case. The pneumonia exclusively affected upper lobes in 8 out of 9 cases. The infection was fatal in 3 cases (mean age 54) through development of septic shock. Early identification and timely treatment of P. Aeruginosa infection is crucial due to its high rate of multi-drug resistance (3). In absence of positive sputum cultures clinical suspicion based on imaging could drastically change patient’s course of illness. Presentation of upper-lobe pneumonia not responding to standard antibiotic regimens should alert clinicians to the differential of P. Aeruginosa infection. Plain radiograph usually gives sufficient information in CAP but a CT scan may be warranted on an individual basis to assess more complex pneumonia.
Giorgi Kiladze MBcHB, MRCP(UK)
Royal Liverpool and Broadgreen University Hospitals NHS Trust
Prescot Street, Liverpool, Merseyside, UK L7 8XP
References
- Rello J, Borgatta B, Lisboa T. Risk factors for Pseudomonas aeruginosa pneumonia in the early twenty-first century. Intensive Care Med. 2013 Dec;39(12):2204-6. [CrossRef] [PubMed]
- Maharaj S, Isache C, Seegobin K, Chang S, Nelson G. Necrotizing Pseudomonas aeruginosa Community-Acquired Pneumonia: A Case Report and Review of the Literature. Case Rep Infect Dis. 2017;2017:1717492. [CrossRef] [PubMed]
- Wolter DJ, Lister PD. Mechanisms of β-lactam resistance among Pseudomonas aeruginosa. Curr Pharm Des. 2013;19(2):209-22.
Abbreviations
- COPD – Chronic Obstructive Pulmonary Disease
- CXR – Chest X-ray
- WBC – White Blood Cells
- CRP – C Reactive Protein
- CURB 65 – Confusion Urea Respiratory rate Blood pressure Age 65
- IV – Intravenous
- AFB – Acid-Fast Bacilli
- HIV – Human Immunodeficiency Virus
- QDS – Quarter Die Sumendum (four times daily)
- CT – Computed Tomography
- L/min – Litres/minute
- CAP – Community Acquired Pneumonia
- HAP – Hospital Acquired Pneumonia
Cite as: Kiladze G. Medical Image of the Month: Cavitating Pseudomonas aeruginosa Pneumonia. Soulthwest J Pulm Crit Care. 2021;23(5):126-8. doi: https://doi.org/10.13175/swjpcc034-21 PDF
November 2021 Imaging Case of the Month: Let’s Not Dance the Twist
Prasad M. Panse MD and Michael B. Gotway MD
Department of Radiology
Mayo Clinic, Arizona
5777 East Mayo Boulevard
Phoenix, Arizona 85054
Editor’s Note: Parts of this presentation were used in the June 2020 Pulmonary Case of the Month.
History of Present Illness: An 82-year-old man presented to his physician for general health maintenance as well as a complaint of persistently poor quality sleep and poor appetite with weight loss. The patient had undergone robotic-assisted radical left nephroureterectomy and cystectomy with pelvic lymph node dissection and urinary diversion for left clear cell renal cell carcinoma (staged T2a, grade 2) and transitional cell carcinoma of the bladder (carcinoma in situ at surgery), approximately 9 months earlier. The patient’s bladder malignancy was initially treated with transurethral resection, with histopathology at that procedure showing high-grade papillary urothelial malignancy with lamina propria invasion, but no muscular invasion; this procedure was followed by formal complete resection approximately 3 months later. The patient’s post-operative course was complicated by significant bleeding which required transfusion of 3 units of blood. He had undergone inferior vena caval filter placement prior to surgery when preoperative testing revealed lower extremity deep venous thrombus and pulmonary embolism.
Past Medical History: The patient’s past medical history was remarkable for atrial fibrillation treated with anticoagulation and hypertension. He also had a history of coronary artery disease and myocardial infarction with moderate systolic dysfunction His medical list included warfarin (for his atrial fibrillation), acetaminophen, vitamin supplementation, hydrochlorothiazide, atorvastatin, ramipril, metoprolol, and zolpidem. He denied allergies. The patient was a former smoker, previously smoking 2 packs-per day for 35 years, quitting over 30 years prior to presentation.
His past surgical history was remarkable for laminectomy in addition to the recent urinary surgery. He also had a history of rectal laceration complicating previous prostatectomy for prostate carcinoma (Gleason 3 + 4, T2).
Physical Examination: showed the patient to be afebrile with normal heart and respiratory rates and blood pressure. Her room air oxygen saturation was 99%. The physical examination did not disclose any salient abnormalities.
Initial Laboratory: The patient’s complete blood count and serum chemistries showed largely normal values, with the white blood cell count was normal at 6.7 x 109 /L (normal, 4-10 x 109 /L). His liver function testing and renal function testing parameters were also within normal limits. Echocardiography showed mildly decreased left ventricular systolic function, but this finding was stable. The patient underwent frontal chest radiography (Figure 1A).

Figure 1. A: Frontal chest radiography. B: Frontal chest radiography performed just over 1 year prior to A shows no specific abnormalities.
Which of the following represents an appropriate interpretation of his frontal chest radiograph? (Click on the correct answer to be directed to the second of fourteen pages).
- Frontal chest radiography shows no specific abnormalities
- Frontal chest radiograph shows a nodule
- Frontal chest radiography shows bilateral interstitial thickening
- Frontal chest radiography shows bilateral pleural effusions
- Frontal chest radiography shows mediastinal and peribronchial lymph node enlargement