
Imaging
Those who care for patients with pulmonary, critical care or sleep disorders rely heavily on chest radiology and pathology to determine diagnoses. The Southwest Journal of Pulmonary, Critical Care & Sleep publishes case-based articles with characteristic chest imaging and related pathology.
The editor of this section will oversee and coordinate the publication of a core of the most important chest imaging topics. In doing so, they encourage the submission of unsolicited manuscripts. It cannot be overemphasized that both radiologic and pathologic images must be of excellent quality. As a rule, 600 DPI is sufficient for radiographic and pathologic images. Taking pictures of plain chest radiographs and CT scans with a digital camera is strongly discouraged. The figures should be cited in the text and numbered consecutively. The stain used for pathology specimens and magnification should be mentioned in the figure legend. Those who care for patients with pulmonary, critical care or sleep disorders rely heavily on chest radiology and pathology to determine diagnoses. The Southwest Journal of Pulmonary, Critical Care & Sleep publishes case-based articles with characteristic chest imaging and related pathology. The editor of this section will oversee and coordinate the publication of a core of the most important chest imaging topics. In doing so, they encourage the submission of unsolicited manuscripts. It cannot be overemphasized that both radiologic and pathologic images must be of excellent quality. As a rule, 600 DPI is sufficient for radiographic and pathologic images. Taking pictures of plain chest radiographs and CT scans with a digital camera is strongly discouraged. The figures should be cited in the text and numbered consecutively. The stain used for pathology specimens and magnification should be mentioned in the figure legend.
December 2023 Medical Image of the Month: Metastatic Pulmonary Calcifications in End-Stage Renal Disease

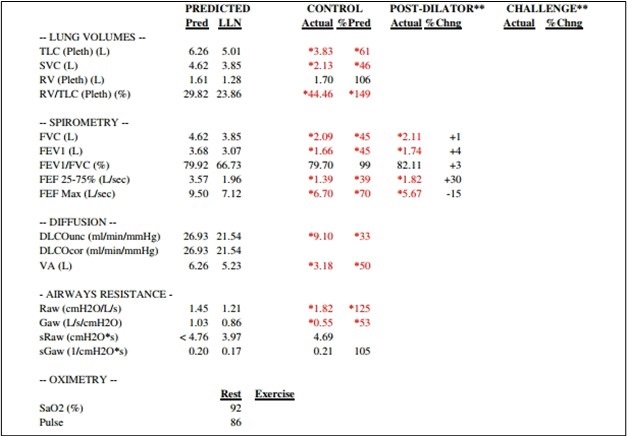
Figure 1. Pulmonary function testing results for the patient demonstrate severe restriction with a reduced diffusion capacity with a corrected DLCO 50% of predicted and FVC 45% of predicted. To view Figure 1 in an enlarged, separate window click here.
{kind=link}
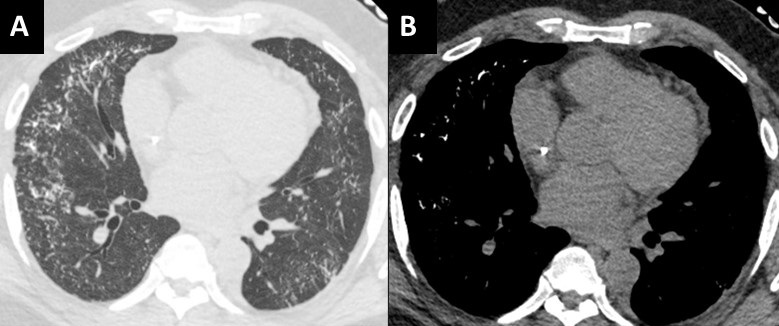
 Figure 2. Unenhanced chest CT images in the axial plane reconstructed with lung (A) and soft tissue (B) display settings. There are innumerable small solid pulmonary nodules with a peripheral distribution, some subpleural sparing, and architectural distortion (A). On soft tissues windows (B) the fact that the nodules are calcified are well-appreciated in the anterior and lateral right mid-lung. To view Figure 2 in a separate, enlarged window click here.
Figure 2. Unenhanced chest CT images in the axial plane reconstructed with lung (A) and soft tissue (B) display settings. There are innumerable small solid pulmonary nodules with a peripheral distribution, some subpleural sparing, and architectural distortion (A). On soft tissues windows (B) the fact that the nodules are calcified are well-appreciated in the anterior and lateral right mid-lung. To view Figure 2 in a separate, enlarged window click here.
{kind=link}
A 51-year-old African-American man with medical history of obesity (BMI 36) and hypertension was seen in pulmonary consultation for preoperative evaluation of kidney transplantation. End-Stage renal disease (ESRD) was diagnosed 7 years before evaluation secondary to resistant hypertension. The patient has been on hemodialysis since then. The patient was on carvedilol, hydralazine, losartan, and calcitriol. He had prescribed sevelamer and prednisone, but he was not taking them. His main symptoms were 3-year chronic dyspnea on exertion and mild morning cough productive of small amounts of clear sputum. He has had no chest pain, wheezes, hemoptysis, fevers, or dizziness. He had trace lower extremity edema. He worked as a forklift operator. He has had no relevant exposures and was a lifetime nonsmoker.
The patient was diagnosed with cryptogenic organizing pneumonia 5 years ago and was on prednisone taper with subjective improvement of symptoms. He has not had lung function testing or biopsies done at that time. He was maintained on 3L oxygen with activity to targets oxygen saturation of 90%. On examination VS: BP 216/100, HR 94, temperature 36.7 °C, SpO2 88 % RA. He was not in respiratory distress. Chest auscultation: symmetrical breath sounds, no added sounds. Examination of the heart, abdomen and rest of the systems were normal. He had trace bilateral pedal edema and clubbing in all digits.
Figure 1 shows his most recent pulmonary function test illustrating a severe restrictive defect with reduced diffusion capacity. Echocardiogram showed ejection fraction of 54%, mild left ventricular hypertrophy and mild diastolic dysfunction. Representative slices of his most recent computed tomography (CT) of the chest are shown in figure 2 and demonstrate multiple scattered small, solid, and calcified pulmonary nodules.
Pulmonary calcifications can either be secondary to hypercalcemia from benign or malignant causes {1}. Such calcification would occur in normal lung tissue due to elevated calcium-phosphate product and is termed metastatic {2,3}. It is thought to occur with higher concentrations of free hydrogen ions, especially in less ventilated areas (West zone 3) with lower pH (more acidotic), leading to calcium-magnesium phosphate compounds (whitlockite-like). Dystrophic calcification on the other hand develops secondary to injury from granulomatous diseases, infections or inherited pulmonary alveolar microlithiasis {4}.
Most cases of metastatic pulmonary calcification are due to ESRD-related hypercalcemia {2}. Most patients are asymptomatic and diagnosed incidentally. Some patients may have non-productive cough, progressive dyspnea, and hypoxia. Lung function testing could show normal or restrictive ventilatory defects, often with impaired diffusion of carbon monoxide. CT scans are diagnostic (Figure 2) and show distinctive diffuse calcifications (sometimes solid and sometimes manifesting as centrilobular ground glass). Bone scintigraphy using technetium-99 diphosphonate scanning would show these calcifications along other parts of the body affected with reported higher sensitivity compared to standard x-ray {5}.
Management is geared towards controlling levels of calcium through phosphate binders, dialysis dosing, and/or parathyroidectomy. Our patient was ultimately evaluated for combined lung/kidney transplantation due to his severe restrictive pulmonary defects.
Abdelmohaymin Abdalla MD1, Clinton Jokerst MD2, Umesh Goswami MD1
Division of Pulmonary and Critical Care Medicine1
Mayo Clinic Arizona, Phoenix, AZ USA
Department of Radiology2
Mayo Clinic Arizona, Phoenix, AZ USA
References
- Kaltreider HB, Baum GL, Bogaty G, McCoy MD, Tucker M. So-called "metastatic" calcification of the lung. Am J Med. 1969 Feb;46(2):188-96. [CrossRef] [PubMed]
- Conger JD, Hammond WS, Alfrey AC, Contiguglia SR, Stanford RE, Huffer WE. Pulmonary calcification in chronic dialysis patients. Clinical and pathologic studies. Ann Intern Med. 1975 Sep;83(3):330-6. [CrossRef] [PubMed]
- Kuzela DC, Huffer WE, Conger JD, Winter SD, Hammond WS. Soft tissue calcification in chronic dialysis patients. Am J Pathol. 1977 Feb;86(2):403-24. [PubMed]
- Chan ED, Morales DV, Welsh CH, McDermott MT, Schwarz MI. Calcium deposition with or without bone formation in the lung. Am J Respir Crit Care Med. 2002 Jun 15;165(12):1654-69. [CrossRef] [PubMed]
- Faubert PF, Shapiro WB, Porush JG, Chou SY, Gross JM, Bondi E, Gomez-Leon G. Pulmonary calcification in hemodialyzed patients detected by technetium-99m diphosphonate scanning. Kidney Int. 1980 Jul;18(1):95-102. [CrossRef] [PubMed]
Cite as: Abdalla A, Jokerst C, Goswami U. December 2023 Medical Image of the Month: Metastatic Pulmonary Calcifications in End-Stage Renal Disease. Southwest J Pulm Crit Care Sleep. 2023;27(6):67-69. doi: https://doi.org/10.13175/swjpccs049-23 PDF
August 2023 Medical Image of the Month: Cannonball Metastases from Metastatic Melanoma
 Figure 1. Upright PA chest radiograph (A) demonstrates innumerable rounded nodules with a slight lower lung predilection. Coronal reconstruction from a subsequent chest CT with contrast (B) confirms innumerable round, solid and non-calcified pulmonary nodules most consistent with a “cannonball” pattern of pulmonary metastatic disease.
Figure 1. Upright PA chest radiograph (A) demonstrates innumerable rounded nodules with a slight lower lung predilection. Coronal reconstruction from a subsequent chest CT with contrast (B) confirms innumerable round, solid and non-calcified pulmonary nodules most consistent with a “cannonball” pattern of pulmonary metastatic disease.
 Figure 2. Axial susceptibility-weighted (A) and pre-contrast T1-weighted (B) images from a brain MRI centered on one (of many) intracranial lesions. This lesion in the posterior right cerebral hemisphere demonstrates a large amount of surrounding susceptibility artifact (A) consistent with blood product, indicating a hemorrhagic metastasis, common in metastatic melanoma which can be very vascular in nature. There is elevated T1 signal surrounding the lesion (B), also consistent with hemorrhage. There is T1 signal in the center of the lesion as well (arrow), which could represent hemorrhage but could also represent melanin, which is T1 bright and can suggest the primary tumor histology (melanoma).
Figure 2. Axial susceptibility-weighted (A) and pre-contrast T1-weighted (B) images from a brain MRI centered on one (of many) intracranial lesions. This lesion in the posterior right cerebral hemisphere demonstrates a large amount of surrounding susceptibility artifact (A) consistent with blood product, indicating a hemorrhagic metastasis, common in metastatic melanoma which can be very vascular in nature. There is elevated T1 signal surrounding the lesion (B), also consistent with hemorrhage. There is T1 signal in the center of the lesion as well (arrow), which could represent hemorrhage but could also represent melanin, which is T1 bright and can suggest the primary tumor histology (melanoma).
A 48-year-old man with a significant smoking history presented with progressive dyspnea, a mildly productive cough with brown-tinged sputum, headache, weight loss, and progressive back pain over a period of 8 weeks. The patient had no known history of lung conditions. As part of their initial evaluation, the patient received a frontal CXR and was found to have innumerable rounded pulmonary nodules throughout the lungs, which were consistent with a “cannonball” pattern of pulmonary metastatic disease (Figure 1A). A subsequent CT confirmed innumerable pulmonary metastases (Figure 1B). An MRI of the brain and spine revealed hemorrhagic brain metastases (Figure 2), spinal metastases, and bone metastases. A biopsy of a lesion in the left iliac bone confirmed the diagnosis of metastatic melanoma.
This case highlights the so-called “cannonball” pattern of pulmonary metastatic disease with innumerable round nodules throughout the lungs with a slight lower lung predilection, consistent with a hematogenous spread of disease to the lungs. Classically, this pattern consists of numerous well-circumscribed relatively large lesions in the lungs with a pattern resembling multiple small "cannonballs". The distribution of nodules is random, and the factors that distinguish a cannonball pattern from a miliary pattern of pulmonary metastatic disease are that cannonball metastases are larger and less numerous compared to a miliary pattern of pulmonary metastatic disease (1,2). Although cannonball pattern of pulmonary metastatic disease is classically described in the setting of metastatic renal cell carcinoma, prostate cancer, choriocarcinoma, and sarcoma, it has been reported for a variety of other primary cancers, including melanoma. Similar cases of late-stage metastatic melanoma presenting as widely metastatic disease of unknown origin has also been reported (3).
Melanoma spreads to the lungs through hematogenous dissemination, resulting in the cannonball (or miliary) lesions observed on imaging. Specifically, when these lesions are small and distributed throughout the lung, they commonly indicate metastatic melanoma. While this classical presentation can be pathognomonic, it is important to consider other potential diagnoses, including malignancy, infectious diseases, and rheumatologic conditions. Malignant causes encompass metastatic colorectal cancer, breast cancer, renal cell carcinoma, choriocarcinoma, prostate carcinoma, and adrenal carcinoma. Additionally, non-cancerous causes include infectious etiologies such as septic emboli, coccidiomycosis, histoplasmosis, miliary tuberculosis, and nocardiosis. It is also important to note that rheumatologic conditions like granulomatosis with polyangiitis (Wegener's granulomatosis) can present with the cannonball sign; however, they typically involve both the upper and lower lungs. In this case, the lesions were determined to be due to metastatic melanoma, which had spread to the lungs via hematogenous dissemination.
For this patient, an oncologist was consulted, who recommended that the patient undergo treatment with ipilimumab and nivolumab. The response rate for this treatment regimen generally exceeds 50%, and more than 50% of individuals continue to survive after 5 years. Frequently, when extensive metastases are observed on imaging, healthcare providers often assume a limited life expectancy and tend to lean towards discussions of hospice care. However, it is important to keep in mind that even in cases of extensive metastatic disease, many cancers can be effectively treated with novel and highly effective immunologic anticancer medications.
Andrew Barsoum MD, Mueez Hussain MD, Ranjit Sivanandham MD, and Sina Bagheri MD.
Southwest Healthcare System
Murrieta, California
References
- Ammannagari N, Polu V. 'Cannon ball' pulmonary metastases. BMJ Case Rep. 2013 Jan 8;2013:bcr2012008158. [CrossRef][PubMed]
- Andreu J, Mauleón S, Pallisa E, Majó J, Martinez-Rodriguez M, Cáceres J. Miliary lung disease revisited. Curr Probl Diagn Radiol. 2002 Sep-Oct;31(5):189-97. [PubMed]
- Lowe A, Bray JJH. Late-stage melanoma presenting with cannonball metastases. BMJ Case Rep. 2020 Dec 12;13(12):e237969. [CrossRef][PubMed]
March 2022 Medical Image of the Month: Pulmonary Nodules in the Setting of Diffuse Idiopathic Pulmonary NeuroEndocrine Cell Hyperplasia (DIPNECH)

Figure 1. Unenhanced chest CT images in the axial plane show solid, non-calcified and well-circumscribed nodules in the right upper lobe (RUL) (A) and lingula (B). The RUL nodule is FDG-avid on axial fused FDG PET-CT image (C) whereas the lingular nodule is not (D).

Figure 2. Unenhanced chest CT images in the axial plane reconstructed with maximum intensity projection (MIP, A) and minimum intensity projection (MinIP, B) techniques show multiple scattered solid pulmonary nodules (arrows) and pulmonary mosaicism consistent with air-trapping (circled). Axial fused images from a 68GA-DOTATATE PET-CT demonstrate some activity in the RUL nodule (C) and more prominent uptake in the lingular nodule (D).

Figure 3. Hematoxylin and Eosin stained low-power pathological image (A) demonstrates the lingular carcinoid tumor (*) as well as several carcinoid tumorlets (arrows) in the adjacent lung. A separate specimen of lung stained with synaptophysin demonstrates multiple tumorlets in the small sample. When taken in conjunction with imaging findings, pathology is in-keeping with a diagnosis of Diffuse Idiopathic Pulmonary Neuroendocrine Cell Hyperplasia (DIPNECH).
A 62-year-old woman presented to an outside hospital with chronic cough, prompting a chest x-ray (CXR). Findings further prompted unenhanced chest CT to evaluate possible pulmonary nodules. The CT demonstrated multiple scattered, solid and centrilobular pulmonary nodules, most of which were small but there were two >1 cm nodules, one in the right upper lobe (RUL) and a second in the lingula (Figure 1A,B). A subsequent FDG PET-CT was performed demonstrating increased metabolic activity in the RUL nodule with no activity in the lingular nodule (Figure 1C,D). Biopsy of the RUL nodule was consistent with a carcinoid. At this point the patient was referred to our center for further management. A repeat chest CT failed to demonstrate any significant change in the nodules. MIP and MinIP reconstructions from that examination demonstrate multiple small, solid pulmonary nodules (arrows) (Figure 2A), many of which were associated with air-trapping resulting in pulmonary mosaicism (circled) (Figure 2B). A 68GA-DOTATATE PET-CT was performed, the results of which provide stark contrast to the FDG-PET in that the RUL nodule demonstrated modest uptake (Figure 2C), whereas the lingular nodule showed very prominent update (Figure 2D). The lingular nodule was resected, H & E-stained pathology image (Figure 3A) demonstrated a typical carcinoid (*) with multiple carcinoid tumorlets in the surgical specimen (arrows). A separate specimen stained with synaptophysin demonstrates multiple neuroendocrine tumorlets. Pathological findings, in conjunction with patient demographics and imaging findings, were consistent with Diffuse Idiopathic Pulmonary NeuroEndocrine Cell Hyperplasia (DIPNECH).
DIPNECH is recognized as a pre-neoplastic lesion in the 2015 WHO classification of lung tumors (1). There is neuroendocrine cell proliferation within the small bronchi and bronchioles which may progress beyond the basement membrane, forming carcinoid tumorlets and in some cases, eventually carcinoid tumors. These airway-centered nodules cause obstruction. In addition, there is often an association between DIPNECH and constrictive bronchiolitis, which causes further airway obstruction (2). The vast majority of patients are women in their 50s-70s and most patients are symptomatic with the most common presenting symptoms being chronic cough and dyspnea (3,4). Many of these patients are often mis-diagnosed with asthma initially (4). The imaging findings of DIPNECH on CT are not specific but can be pathognomonic in some cases. There are almost always innumerable small solid (and sometimes ground glass) centrilobular nodules and nodular bronchial thickening with associated pulmonary mosaicism related to air trapping. Nodules are either stable or very slowly growing over years with the largest nodules usually being biopsied or resected and yielding typical carcinoid on pathology (4). A relatively new nuclear medicine imaging study, 68Ga-DOTATATE PET-CT, shows promise as a higher resolution and more sensitive examination for detection of neuroendocrine tumors (relative to octreotide scans), including pulmonary carcinoid tumors in the setting of DIPNECH (5,6).
Clinton Jokerst MD1, Henry Tazelaar2, Carlos Rojas MD1, Prasad Panse MD1, Kris Cummings MD1, Eric Jensen MD1 and Michael Gotway MD1
Departments of Radiology1 and Pathology2
Mayo Clinic Arizona, Scottsdale, AZ USA
References
- Gosney JR, Austin JHM, Jett J, et al. Diffuse pulmonary neuroendocrine cell hyperplasia. In: Travis WD, Brambilla E, Burke AP, et al., eds. WHO classification of tumours of the lung, pleura, thymus and heart. Lyon, IARC Press, 2015; pp. 78-79.
- Samhouri BF, Azadeh N, Halfdanarson TR, Yi ES, Ryu JH. Constrictive bronchiolitis in diffuse idiopathic pulmonary neuroendocrine cell hyperplasia. ERJ Open Res. 2020 Nov 16;6(4):00527-2020. [CrossRef] [PubMed]
- Rossi G, Cavazza A, Spagnolo P, Sverzellati N, Longo L, Jukna A, Montanari G, Carbonelli C, Vincenzi G, Bogina G, Franco R, Tiseo M, Cottin V, Colby TV. Diffuse idiopathic pulmonary neuroendocrine cell hyperplasia syndrome. Eur Respir J. 2016 Jun;47(6):1829-41. [CrossRef] [PubMed]
- Little BP, Junn JC, Zheng KS, Sanchez FW, Henry TS, Veeraraghavan S, Berkowitz EA. Diffuse Idiopathic Pulmonary Neuroendocrine Cell Hyperplasia: Imaging and Clinical Features of a Frequently Delayed Diagnosis. AJR Am J Roentgenol. 2020 Dec;215(6):1312-1320. [CrossRef] [PubMed]
- Deppen SA, Blume J, Bobbey AJ, Shah C, Graham MM, Lee P, Delbeke D, Walker RC. 68Ga-DOTATATE Compared with 111In-DTPA-Octreotide and Conventional Imaging for Pulmonary and Gastroenteropancreatic Neuroendocrine Tumors: A Systematic Review and Meta-Analysis. J Nucl Med. 2016 Jun;57(6):872-8. [CrossRef] [PubMed]
- Fraum TJ, Ritter JH, Chen DL. Diffuse Idiopathic Pulmonary Neuroendocrine Cell Hyperplasia on Somatostatin Receptor Imaging. Am J Respir Crit Care Med. 2018 Nov 1;198(9):1223-1225. [CrossRef] [PubMed]
Cite as: Jokerst C, Tazelaar H, Rojas C, Panse P, Cummings K, Jensen E, Gotway M. March 2022 Medical Image of the Month: Pulmonary Nodules in the Setting of Diffuse Idiopathic Pulmonary Neuroendocrine Cell Hyperplasia (DIPNECH). Southwest J Pulm Crit Care Sleep;2022:40-42. doi: https://doi.org/10.13175/swjpccs010-22 PDF
February 2022 Medical Image of the Month: Multifocal Micronodular Pneumocyte Hyperplasia in the Setting of Tuberous Sclerosis

Figure 1. Unenhanced chest CT in the axial (A) plane showing multiple subsolid pulmonary nodules in a random distribution (arrows). Unenhanced chest CT in the axial (A) plane compared to an image from a contrast-enhanced abdominal CT performed 1 year earlier (B) shows relative stability of these nodules (arrows). In a 22 y/o man with known Tuberous Sclerosis Complex, these findings are consistent with Multifocal Micronodular Pneumocyte Hyperplasia. Click here to view Figure 1 in an enlarged window.
{kind=link}

Figure 2. Unenhanced chest CT in the axial (A) plane, soft tissue window display settings, demonstrate foci of myocardial fat (arrow). Unenhanced chest CT in the axial (B) and sagittal (C) planes, bone window display settings, shows multiple small scattered sclerotic osseous foci (circles). These ancillary findings are quite common in the setting of tuberous sclerosis. Click here to view Figure 2 in an enlarged window.
{kind=link}
A 22-year-old man with a known diagnosis of Tuberous Sclerosis Complex (TSC) presents for a follow-up unenhanced chest CT to re-evaluate pulmonary nodules seen in the lung bases on a prior abdominal CT. The patient also has a history of multiple renal lesions consistent with lipid-poor angiomyolipomas based on previous abdominal MRI findings. The chest CT demonstrated multiple scattered, randomly distributed sub-centimeter pulmonary nodules of solid or subsolid morphology [Figure 1A]. Those nodules visible in the lung bases on the prior abdominal CT had remined stable over the 12-month interval consistent with multifocal microscopic pneumocyte hyperplasia (MMPH)[Figure 1B,C]. Myocardial fatty foci (MFF) were visualized in the heart on soft tissue window display settings [Figure 2A] as were multiple scattered sclerotic bone lesions on bone window display settings [Figure 2B,C]. No pulmonary cysts were seen to suggest lymphangioleiomyomatosis (LAM) and there were no thoracic lymphangiomas.
MMPH represents a benign hamartomatous proliferation of type II pneumocytes which manifest as small, randomly scattered pulmonary nodules that can be solid or subsolid and are self-limited (1). MMPH is rare in general, but quite common in TSC with a reported incidence as high as 71% (2). MMPH does not demonstrate a sex predilection (unlike LAM in TSC). It is important to remember MMPH in the setting of TSC as it represents a “don’t touch” lesion; recognizing it as such can save unnecessary trouble for the patient (3). The MFF seen on this chest CT also is a relatively common and specific finding in TSC, seen in at least 50% of TSC patients (4,5). Although MMPH and MFF appear to be relatively specific imaging findings in the setting of TSC, as of yet they have not been incorporated into the diagnostic criteria for TSC (6). The small sclerotic bone lesions, especially involving the posterior elements of the spine, are also a well described finding in TSC; however, this finding is much less specific and can be seen in many conditions (7).
Clinton Jokerst MD, Carlos Rojas MD, Prasad Panse MD, Kris Cummings MD, Eric Jensen MD and Michael Gotway MD
Department of Radiology
Mayo Clinic Arizona
Scottsdale, AZ USA
References
- Franz DN, Brody A, Meyer C, Leonard J, Chuck G, Dabora S, Sethuraman G, Colby TV, Kwiatkowski DJ, McCormack FX. Mutational and radiographic analysis of pulmonary disease consistent with lymphangioleiomyomatosis and micronodular pneumocyte hyperplasia in women with tuberous sclerosis. Am J Respir Crit Care Med. 2001 Aug 15;164(4):661-8. [CrossRef] [PubMed]
- Wataya-Kaneda M, Tanaka M, Hamasaki T, Katayama I. Trends in the prevalence of tuberous sclerosis complex manifestations: an epidemiological study of 166 Japanese patients. PLoS One. 2013 May 17;8(5):e63910. [CrossRef] [PubMed]
- Aswani Y, Gavai B. Multifocal micronodular pneumocyte hyperplasia: A "touch-me-not" pulmonary lesion in tuberous sclerosis complex. Lung India. 2018 Sep-Oct;35(5):445-446. [CrossRef] [PubMed]
- Adriaensen ME, Schaefer-Prokop CM, Duyndam DA, Zonnenberg BA, Prokop M. Fatty foci in the myocardium in patients with tuberous sclerosis complex: common finding at CT. Radiology. 2009 Nov;253(2):359-63. [CrossRef] [PubMed]
- Tresoldi S, Munari A, Di Leo G, Pompili G, Magistrelli P, Secchi F, La Briola F, Canevini MP, Cornalba G, Sardanelli F. Myocardial Fatty Foci in Adult Patients with Tuberous Sclerosis Complex: Association with Gene Mutation and Multiorgan Involvement. Radiology. 2015 Nov;277(2):398-405. [CrossRef] [PubMed]
- Northrup H, Krueger DA; International Tuberous Sclerosis Complex Consensus Group. Tuberous sclerosis complex diagnostic criteria update: recommendations of the 2012 Iinternational Tuberous Sclerosis Complex Consensus Conference. Pediatr Neurol. 2013 Oct;49(4):243-54. [CrossRef] [PubMed]
- Baskin HJ Jr. The pathogenesis and imaging of the tuberous sclerosis complex. Pediatr Radiol. 2008 Sep;38(9):936-52. [CrossRef] [PubMed]
May 2019 Imaging Case of the Month: Asymptomatic Pulmonary Nodules and Cysts in a 47-Year-Old Woman
Michael B. Gotway, MD
Department of Radiology
Mayo Clinic Arizona
Scottsdale, AZ USA
Clinical History: A 47-year-old previously healthy woman presented to her new physician for a routine physical examination. The patient had no complaints. The patient’s physical examination showed normal vital signs and clear lungs; the physical examination was essentially unremarkable. The patient’s past medical history included a brief smoking history, having quit over 20 years earlier, as well as seasonal allergies. Her past surgical history included an appendectomy nearly 20 years earlier and a hysterectomy for bleeding related to uterine leiomyomas approximately 12 years prior to presentation. The patient was not taking any prescription medications.
Basic laboratory data, including a complete blood count, electrolyte panel, and liver function studies were all within the normal range. An electrocardiogram revealed normal findings. Frontal and lateral chest radiography (Figure 1) was performed.

Figure 1. Frontal (A) and lateral (B) chest radiography.
Which of the following statements regarding the chest radiograph is most accurate? (click on the correct answer to be directed to the second of eleven pages)
- The chest radiograph shows mediastinal and hilar lymph node enlargement
- The chest radiograph shows multifocal nodular pulmonary consolidation
- The chest radiograph shows multiple, bilateral cavitary nodules
- The chest radiograph shows multiple, bilateral circumscribed nodules
- The chest radiograph shows nodular interstitial thickening
Cite as: Gotway MB. May 2019 imaging case of the month: Asymptomatic pulmonary nodules and cysts in a 47-year-old woman. Southwest J Pulm Crit Care. 2019;18(5):106-19. doi: https://doi.org/10.13175/swjpcc022-19 PDF
Medical Image Of The Week: Septic Pulmonary Emboli Misdiagnosed As Metastatic Disease

Figure 1. Representative thoracic CT axial images showing multiple pulmonary nodules (red arrows).
A 54-year-old previously healthy man presented with acute onset of left-sided, sharp pleuritic chest pain and dry cough. He denied having fever, hemoptysis, shortness of breath, or unintentional weight loss. Review of system was positive for bright blood per rectum for the last year. He had a root canal procedure done 3 weeks prior to presentation. His is a 30 pack-year smoker, drinks alcohol occasionally, but denied any IV drug use.
On admission, he was afebrile and hemodynamically stable. Clinical examination was positive for fecal occult blood test. CBC revealed WBC of 12,800/mm3 and his hemoglobin was11.9 g/dL. Thoracic CT scan with contrast was negative for pulmonary embolism, but showed multiple bilateral pulmonary nodules suspicious for malignancy (Figure 1). The left upper lobe showed a subpleural 2.4 x 1.5 cm rounded opacity and emphysematous changes. CT of the abdomen and pelvis showed folds in the stomach but was otherwise unremarkable.
Esophagogastroduodenoscopy was negative. Colonoscopy showed non-bleeding internal hemorrhoids. He underwent percutaneous CT guided lung biopsy. Pathology report showed distended alveoli filled with polymorphonuclear leukocytes mixed with fibrin consistent with septic emboli and no evidence of malignancy. Special stains for organisms were negative. Blood cultures were negative, Trans-esophageal echocardiograph was normal. Mandibular film done was negative for dental abscess. HIV serology, Quantiferon gold, ß-d glucan, Aspergillus, and mycobacterial culture of sputum were negative. During his hospital stay he developed a fever and his WBC count increased. He was empirically started on broad spectrum antibiotics and he clinically improved significantly.
Septic pulmonary embolus (SPE) is a serious and uncommon condition that poses a diagnostic challenge and carries a high mortality (1,2). Presenting symptoms are often non-specific. Blood cultures may be negative initially. Similarly, chest radiography is not helpful to establish a diagnosis. CT is more useful, usually showing multiple peripheral nodular opacities. SPE can be suspected by the presence of potential source of underlying infection, febrile illness and multiple pulmonary nodules.
Dima Dandachi MD and Sathish Krishnan MD
Department of Internal Medicine
Saint Francis Hospital
Evanston, IL
References
-
Ye R, Zhao L, Wang C, Wu X, Yan H. Clinical characteristics of septic pulmonary embolism in adults: a systematic review. Respir Med 2014;108(1):1-8. [CrossRef] [PubMed]
-
Shiota Y, Taniguchi A, Yuzurio S, Horita N, Hosokawa S, Watanabe Y, Tohmori H, Ono T; Okayama Respiratory Disease Study Group. Septic pulmonary embolism induced by dental infection. Acta Med Okayama. 2013;67(4):253-8. [PubMed]
Reference as: Dandachi D, Krishnan S. Medical image of the week: septic pulmonary emboli misdiagnosed as metastatic disease. Southwest J Pulm Crit Care. 2014;9(1):38-9. doi: http://dx.doi.org/10.13175/swjpcc083-14 PDF
Medical Image of the Week: Parietal Mass

Figure 1. MRI of the head with contrast. Panel A: A 2.2 cm X 2.1 cm enhancing mass within the right precuneus with surrounding vasogenic edema. Panel B: Coronal view.
A 48 year old man presented to the emergency department with a witnessed tonic clonic seizure by family members and 1 week worsening headaches and gait ataxia. Non-contrast CT of the head showed a large right-sided parietal mass. MRI of the head was done to further evaluate the mass (Figure 1). CT chest/abdomen/pelvis showed bilateral pulmonary nodules, mediastinal lymphadenopathy, hepatic lesions, and thickening of the mid-distal esophagus. The patient was evaluated by neurology and started on dexamethasone and levetiracetam. Neurosurgery was consulted and performed a right-sided craniotomy and parietal mass resection. Later, an EGD was performed and biopsies were taken of the esophagus. The patient was found to have metastatic esophageal adenocarcinoma.
Andrew I. Kovoor MD and Sudhir Kumar Tutiki MD
Department of Medicine
University of Arizona
Tucson, Arizona
Reference as: Kovoor AI, Tutiki SK. Medical image of the week: parietal mass. Southwest J Pulm Crit Care. 2014;8(5):290. doi: http://dx.doi.org/10.13175/swjpcc045-14 PDF
Medical Image of the Week: Metastatic Melanoma with Hemorrhage

Figure 1. Axial image of CT Chest with contrast showing pulmonary metastatic masses and alveolar opacities consistent with pulmonary hemorrhage.

Figure 2. Coronal image of CT Chest with contrast showing innumerable pulmonary nodules and masses along with ground-glass alveolar opacities representing alveolar hemorrhage.
A 62 year-old gentleman presented with right leg swelling due to an extensive DVT in the right femoral vein. He was found to have a right groin mass attributed to metastatic malignant melanoma. Chest X-ray and CT revealed multiple bilateral pulmonary nodules. He was started on warfarin 3mg daily for acute DVT and referred to Oncology. 2 weeks later he developed hemoptysis and was found to be hypoxemic. He was admitted to our MICU. His INR upon admission was 8.2 and hemoglobin 6.4. CT Chest showed innumerable bilateral pulmonary nodules and ground-glass alveolar opacities with thickening and nodularity of intra-lobular septa adjacent to the nodules. Warfarin was held and packed RBC and FFP transfusions were given with progressive improvement in hemoptysis and pulmonary status.
Tauseef Afaq Siddiqi, MD; Abdulmajid Eddib, MD; Phillip Factor, DO; and Steven Knoper, MD
Department of Medicine
Section of Pulmonary, Allergy, Critical Care and Sleep Medicine
The University of Arizona
Tucson, AZ 85724, USA
Reference as: Siddiqi TA, Eddib A, Factor P, Knoper S. Medical image of the week: metastatic melanoma with hemorrhage. Southwest J Pulm Crit Care. 2013;6(6):287-8. http://dx.doi.org/10.13175/swjpcc079-13 PDF
Medical Image of the Week: Amyloidosis
A 60-year-old man with multiple pulmonary calcified nodules and masses was found to have nodular pulmonary light chain amyloidosis with a G kappa light chain in serum. He underwent stem cell transplant in 2003. In 2009, he was found to have pulmonary hypertension. Despite therapy, pulmonary hypertension and amyloidosis progressed.


Figure 1: Axial CT scan of the chest, lung and mediastinal windows, showing multiple calcified pulmonary nodules and masses secondary to Amyloidosis
Steven Knoper, MD; Carmen Luraschi-Monjagatta, MD and Aarthi Ganesh, MD
Division of Pulmonary, Allergy, Critical Care and Sleep Medicine
Arizona Respiratory Center
University of Arizona
Tucson, Arizona
Refernce as: Knoper S, Luraschi-Monjagatta C, Ganesh A. Medical image of the week: amyloidosis. Southwest J Pulm Crit Care 2013;6(1):52. PDF