
Imaging
Those who care for patients with pulmonary, critical care or sleep disorders rely heavily on chest radiology and pathology to determine diagnoses. The Southwest Journal of Pulmonary, Critical Care & Sleep publishes case-based articles with characteristic chest imaging and related pathology.
The editor of this section will oversee and coordinate the publication of a core of the most important chest imaging topics. In doing so, they encourage the submission of unsolicited manuscripts. It cannot be overemphasized that both radiologic and pathologic images must be of excellent quality. As a rule, 600 DPI is sufficient for radiographic and pathologic images. Taking pictures of plain chest radiographs and CT scans with a digital camera is strongly discouraged. The figures should be cited in the text and numbered consecutively. The stain used for pathology specimens and magnification should be mentioned in the figure legend. Those who care for patients with pulmonary, critical care or sleep disorders rely heavily on chest radiology and pathology to determine diagnoses. The Southwest Journal of Pulmonary, Critical Care & Sleep publishes case-based articles with characteristic chest imaging and related pathology. The editor of this section will oversee and coordinate the publication of a core of the most important chest imaging topics. In doing so, they encourage the submission of unsolicited manuscripts. It cannot be overemphasized that both radiologic and pathologic images must be of excellent quality. As a rule, 600 DPI is sufficient for radiographic and pathologic images. Taking pictures of plain chest radiographs and CT scans with a digital camera is strongly discouraged. The figures should be cited in the text and numbered consecutively. The stain used for pathology specimens and magnification should be mentioned in the figure legend.
January 2025 Medical Image of the Month: Psoriasis with Pulmonary Involvement

Figure 1. Axial lung-windowed CT reconstructions through the mid (A,B) and lower (C) lungs from a 58-year-old man with psoriasis presenting for evaluation of interstitial lung disease. There is peripheral and lower lung predominant reticulation, ground glass, and traction bronchiolectasis with architectural distortion and atelectasis. To view Figure 1 in a separate enlarged window click here.

{kind=link}
Figure 2. Low-power (A) and high-power (B,C) hematoxylin & eosin-stained pathology slides from a surgical lung biopsy (left lower lobe) demonstrating scattered lymphoid aggregates with patchy granulomatous organizing pneumonia and scattered loosely formed nonnecrotizing granulomas, concern for underlying systemic connective tissue disease-related interstitial lung disease. To view Figure 2 in a separate enlarged window click here.
{kind=link}
A 58-year-old man presented to our pulmonary service for a second opinion concerning his interstitial lung disease (ILD), which had been diagnosed as rheumatoid arthritis associated ILD. The patient had a positive rheumatoid factor (barely) at an outside institution, but no other test results or historical or physical exam findings to suggest rheumatoid arthritis. He was being treated with mycophenolate, but did not feel that he was improving. To the contrary, there had been a recent decline in his overall lung function. The only other relevant medical history is psoriasis. The patient is a lifelong nonsmoker. Resting pulse oximetry was 95% on room air with a brief desaturation to 88% during ambulation, which quickly recovered with rest. The patient’s vital signs were otherwise normal. Physical exam findings were normal aside from mild cutaneous findings of plaque psoriasis. Results from pulmonary function testing at an outside institution were available, revealing a forced vital capacity 40% of reference and DLCO 37% of reference. The overall picture was consistent with restrictive lung disease. Images from an outside CT (Figure 1) demonstrated patchy findings of ILD with peripheral and lower lobe predominant reticulation, ground glass, and architectural distortion without any significant honeycombing or air trapping. The pattern was felt to be pretty nonspecific, but most consistent with ILD in the setting of autoimmune disease, favoring an NSIP or OP pattern over UIP.
Slides from the patient’s outside surgical lung biopsy were reviewed by our pathology department, who have expertise regarding pulmonary manifestations of psoriasis (1). Pathology (Figure 2) showed randomly distributed lymphoid aggregates in association with mild patchy chronic inflammatory infiltrates and patchy areas of numerous macrophages filling airspaces. There were scattered foci of organizing pneumonia focally with nonnecrotizing granulomas. In addition, there were a few scattered very loosely formed nonnecrotizing granulomas. Rare eosinophils were also present. Rare foci of osseous metaplasia were also identified. While the findings were felt to be nonspecific, they are most concerning for an underlying systemic connective tissue disease involving the lung. The case was discussed at our multidisciplinary ILD conference and a consensus diagnosis of ILD related to psoriasis was made. There is limited data suggesting possible improvement in psoriatic ILD with psoriasis treatment using secukinumab (2). However, there are also reports of secukinumab exacerbating ILD in the setting of psoriasis (3). Given the patient’s lack of improvement on mycophenolate, a trial of secukinumab is being considered.
Interstitial pneumonia is relatively rare in the setting of psoriasis, with a series of 392 psoriasis patients demonstrating an incidence of 2% (4). In this series, the most common imaging findings were lower lung predominate ground glass and reticulation, as was seen in this case. Interestingly, one case series (5) found that a UIP pattern of fibrosis was the most common pattern of ILD on CT in patients with plaque psoriasis; however, many of these patients were smokers. Concomitant smoking seems to predispose the patient towards a UIP pattern of ILD in the setting of psoriasis. In non-smokers, NSIP and OP patterns of ILD seemed more prevalent. Although rare, ILD in psoriasis is an important possibility to consider given that some patients treated with biologic agents for their psoriasis experienced improvements in their ILD (2,4).
Clint Jokerst, MD1, Yasmeen M. Butt, MD2
Departments of 1Radiology and 2Pathology
Mayo Clinic Arizona
Phoenix, AZ USA
References
Butt YM, Smith ML, Tazelaar HD, Roden AC, Mengoli MC, Larsen BT. Surgical Pathology of Diffuse Parenchymal Lung Disease in Patients With Psoriasis or Psoriatic Arthritis. Arch Pathol Lab Med. 2022 May 1;147(5):525-533. [CrossRef][PubMed]
Miyachi H, Nakamura Y, Nakamura Y, Matsue H. Improvement of the initial stage of interstitial lung disease during psoriasis treatment with secukinumab. J Dermatol. 2017 Dec;44(12):e328-e329. [CrossRef][PubMed]
Kajihara I, Yamada-Kanazawa S, Maeda-Otsuka S, Jinnin M, Akaike K, Ihn H. Secukinumab-induced interstitial pneumonia in a patient with psoriasis vulgaris. J Dermatol. 2017 Dec;44(12):e322-e323. [CrossRef][PubMed]
Kawamoto H, Hara H, Minagawa S, Numata T, Araya J, Kaneko Y, Umezawa Y, Asahina A, Nakagawa H, Kuwano K. Interstitial Pneumonia in Psoriasis. Mayo Clin Proc Innov Qual Outcomes. 2018 Sep 20;2(4):370-377. [CrossRef][PubMed]
Rizzetto G, Tagliati C, Fogante M, et al. CT Patterns of Interstitial Lung Disease in Patients with Plaque Psoriasis: A Retrospective Case Series Study. Medicina (Kaunas). 2023 Sep 12;59(9):1650. [CrossRef][PubMed]
Cite as: Jokerst C, Butt YM. January 2025 Medical Image of the Month: Psoriasis with Pulmonary Involvement. Southwest J Pulm Crit Care Sleep. 2025;30(1):5-7. doi:
December 2024 Medical Image of the Month: An Endobronchial Tumor

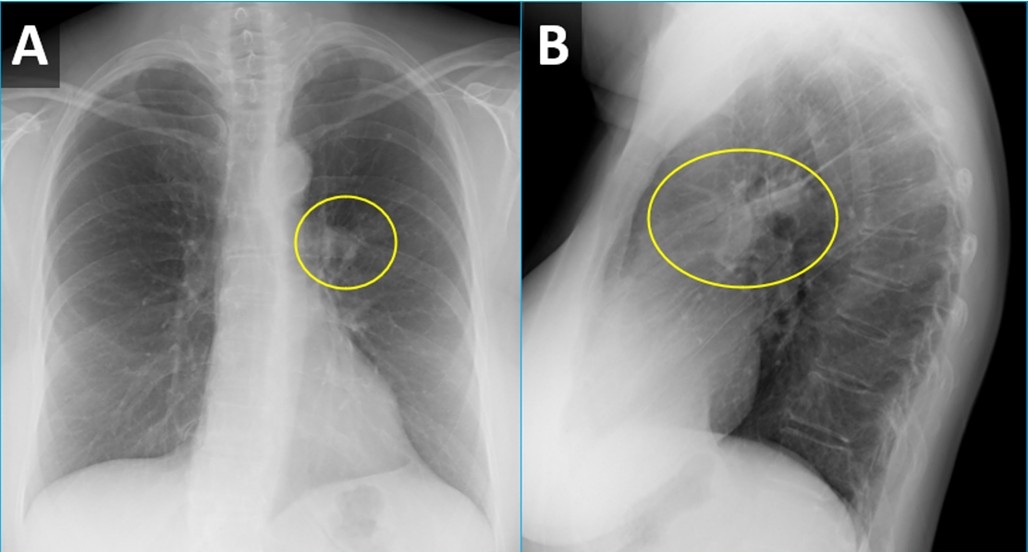
Figure 1. PA (A) and lateral (B) CXR from a woman with wheezing demonstrating a right perihilar nodule projecting within the lingula (circled) with associated atelectasis. To view Figure 1 in a separate, enlarged window click here.
{kind=link}
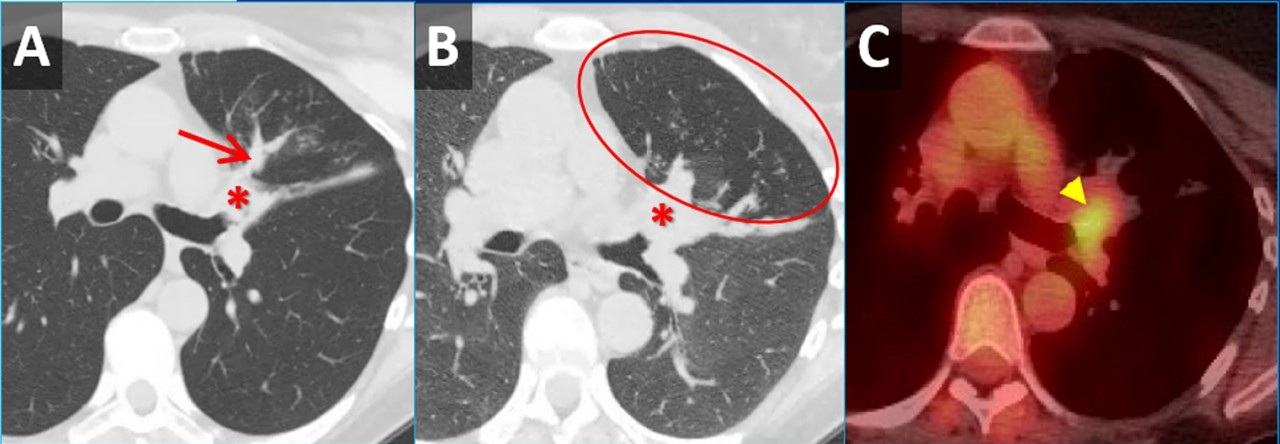
 Figure 2. Inspiratory (A) and expiratory (B) axial CT images demonstrating a mass obstructing the lingular bronchus (*) with post-obstructive mucus plugging (arrow) and air-trapping (circled). Axial image from an FDG PET-CT (C) demonstrates moderate FDG uptake within the nodule (arrowhead). No other areas of tracer uptake were seen to suggest nodal metastatic disease. To view Figure 2 in a separate, enlarged window click here.
Figure 2. Inspiratory (A) and expiratory (B) axial CT images demonstrating a mass obstructing the lingular bronchus (*) with post-obstructive mucus plugging (arrow) and air-trapping (circled). Axial image from an FDG PET-CT (C) demonstrates moderate FDG uptake within the nodule (arrowhead). No other areas of tracer uptake were seen to suggest nodal metastatic disease. To view Figure 2 in a separate, enlarged window click here.
{kind=link}
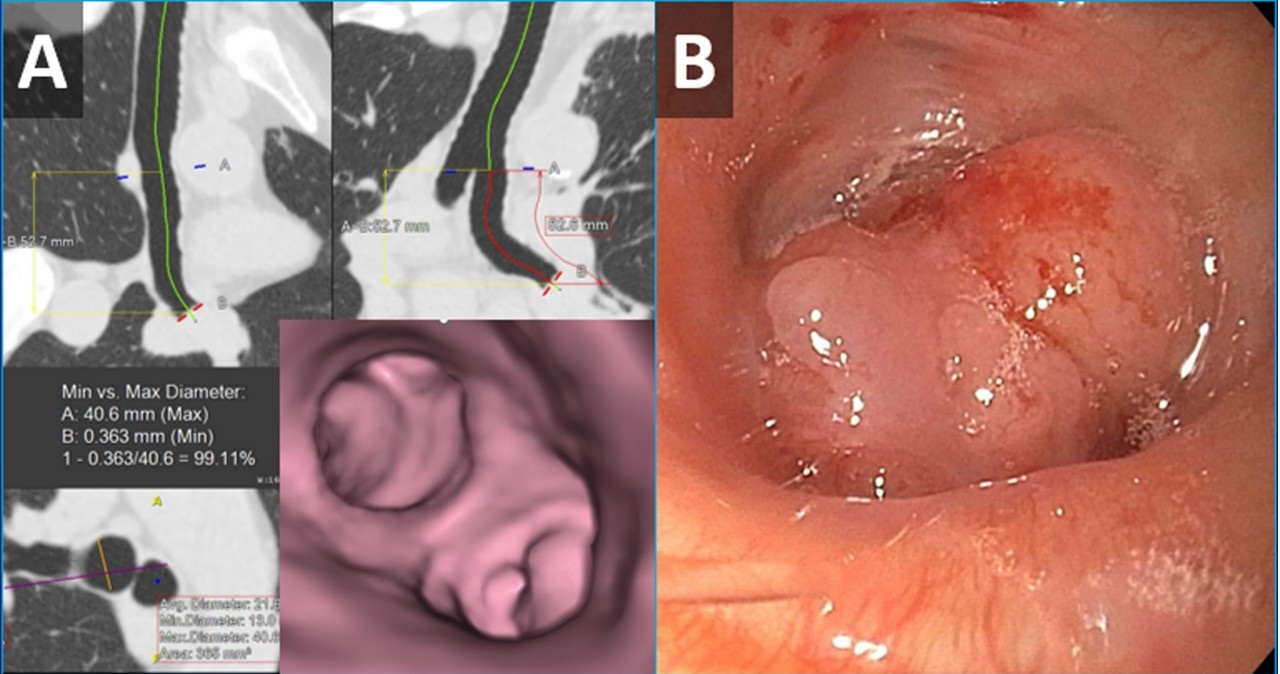
 Figure 3. Images from virtual bronchoscopic reconstructions from the patient’s CT (A) demonstrating a nodule obstructing the lingular bronchus. Image from bronchoscopy (B) obtained just prior to biopsy correlates nicely with virtual bronchoscopic findings. To view Figure 3 in a separate, enlarged window click here.
Figure 3. Images from virtual bronchoscopic reconstructions from the patient’s CT (A) demonstrating a nodule obstructing the lingular bronchus. Image from bronchoscopy (B) obtained just prior to biopsy correlates nicely with virtual bronchoscopic findings. To view Figure 3 in a separate, enlarged window click here.
{kind=link}
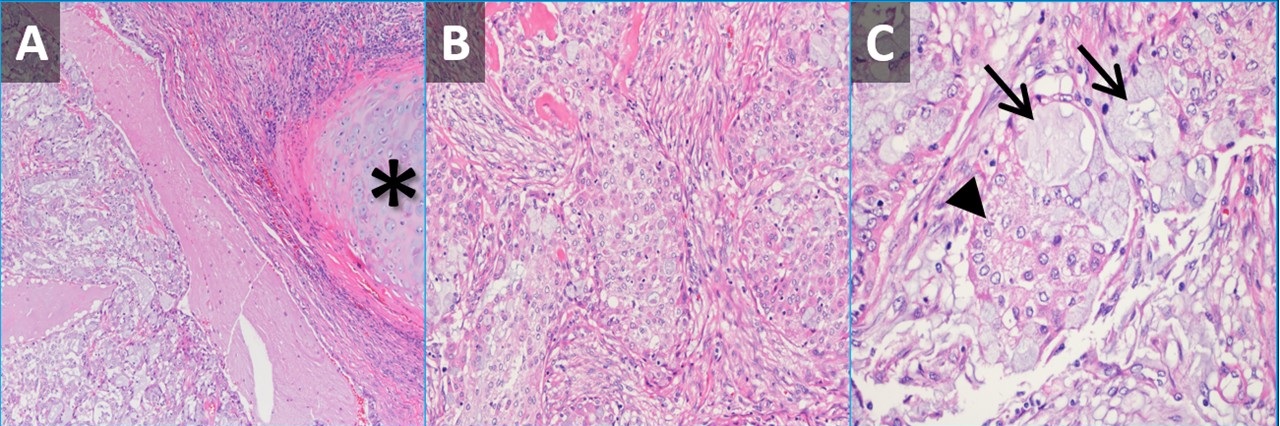
 Figure 4. Low-power (A) and high-power (B,C) hematoxylin & eosin-stained pathology slides from the nodule demonstrating submucosal tumor adjacent to airway cartilage (*). The tumor contains some squamoid-appearing cells (B) as well as some mucinous cells (C, arrows) and intermediate-appearing cells (C, arrowhead). To view Figure 4 in a separate, enlarged window click here.
Figure 4. Low-power (A) and high-power (B,C) hematoxylin & eosin-stained pathology slides from the nodule demonstrating submucosal tumor adjacent to airway cartilage (*). The tumor contains some squamoid-appearing cells (B) as well as some mucinous cells (C, arrows) and intermediate-appearing cells (C, arrowhead). To view Figure 4 in a separate, enlarged window click here.
{kind=link}
A 61-year-old woman was for wheezing. She reported that the symptoms were sudden in onset and persisted for 2 months without improvement. There was no infectious prodrome, no history of an aspiration event, and the symptoms had no exacerbating or relieving factors. The patient reported a past medical history of reflux (controlled on omeprazole), dyslipidemia, hypertension, and migraine headaches. Her past surgical history includes remote histories of breast augmentation, hysterectomy and salpingo-oophorectomy, cholecystectomy, and urethral sling. The patient was a never-smoker with no history of illicit drug use, travel, or exposures. Family history was non-contributory. The patient medications included Crestor, Thiazide, Imitrex, Losartan, and Omeprazole. No known drug allergies.
Her vital signs were normal. Physical exam demonstrated an inspiratory wheeze which was diffuse and best appreciated anteriorly. A PA and Lateral chest x-ray was done at the time of initial referral (Figure 1). A CT scan was subsequently obtained (Figure 2), the results of which led to a PET-CT (Figure 2) and, eventually, bronchoscopy with biopsy (Figure 3). Pathological results were consistent with a low-grade mucoepidermoid carcinoma (MEC) (Figure 4). The patient subsequently underwent left upper lobectomy with lymph node dissection. Surgical pathology demonstrated a 2.5 cm well-differentiated MEC with negative margins; all sampled lymph nodes were negative for malignancy.
MEC in the lungs is rare, accounting for 0.1%-0.2% of pulmonary malignancies (1). These tumors are thought to arise from minor salivary glands in the tracheobronchial tree (2). They are classified as low grade or high grade based on histological criteria (3). On imaging, these tumors are more common in lobar or segmental airways and tend to be round or lobular with well-circumscribed margins. They tend to be vascular and demonstrate heterogeneous enhancement on contrast-enhanced CT. Because they arise from the lining of the airways, they are often associated with post-obstructive findings like mucus plugging, air-trapping, atelectasis, and pneumonia. Patients usually present with symptoms related to endoluminal growth, including persistent cough/sputum, wheezing, dyspnea, hemoptysis, and/or recurrent pneumonias. Patients are often initially mis-diagnosed with asthma, bronchitis, or COPD. The patients frequently do not have a smoking history, which can be helpful when ordering a differential diagnosis. The lesions often demonstrate submucosal growth so bronchial washings/brushings are often negative, as was the case for this patient. This case is a good reminder of the “other” endobronchial tumors, which also include carcinoid tumors (well-circumscribed, vascular, more common in bronchi as opposed to trachea), adenoid cystic carcinoma (usually involve the trachea as a “cylindroma”, have submucosal and perineural growth), sarcomas (chondrosarcoma, sarcoma metastases), hamartomas (often contain fat and/or popcorn calcifications), and tracheobronchial papillomatosis (younger patients, multiple cavitary lesions) (4).
Clinton E. Jokerst MD, Matthew T. Stib MD, Carlos Rojas MD, Michael B. Gotway MD
Department of Radiology
Mayo Clinic Arizona
Phoenix, AZ USA
References
- Miller DL, Allen MS. Rare pulmonary neoplasms. Mayo Clin Proc. 1993 May;68(5):492-8. doi: [CrossRef] [PubMed]
- Ishizumi T, Tateishi U, Watanabe S, Maeda T, Arai Y. F-18 FDG PET/CT imaging of low-grade mucoepidermoid carcinoma of the bronchus. Ann Nucl Med. 2007 Jul;21(5):299-302. [CrossRef][PubMed]
- Yousem SA, Hochholzer L. Mucoepidermoid tumors of the lung. Cancer. 1987 Sep 15;60(6):1346-52. [CrossRef] [PubMed]
- Park CM, Goo JM, Lee HJ, Kim MA, Lee CH, Kang MJ. Tumors in the tracheobronchial tree: CT and FDG PET features. Radiographics. 2009 Jan-Feb;29(1):55-71. [CrossRef] [PubMed]
August 2024 Imaging Case of the Month: An Unexplained Pleural Effusion
Michael B. Gotway MD
Department of Radiology
Mayo Clinic, Arizona
Scottsdale, AZ USA
Clinical History: A 65-year-old woman with presents with intermittent right-sided chest pain and shortness of breath / dyspnea on exertion for several months’ duration.
The patient’s past medical history includes a history of myocardial infarction with stent placement and atrial fibrillation. She has no prior surgical history aside from carpal tunnel release and tonsillectomy.
The patient is a lifelong non-smoker, she reports no allergies and she drinks alcohol only socially and denies illicit drug use. Her medications include Xarelto (rivaroxaban) for her atrial fibrillation, alendronate, atorvastatin, metoprolol, and pantoprazole in addition to a multivitamin.
On physical examination the patient was obese but not in acute distress, with normal blood pressure, pulse rate, and respiratory rate. Her pulmonary and cardiovascular examination was unremarkable aside for dullness to percussion over the right posterior and lateral thorax, and her musculoskeletal examination did not disclose any abnormalities. She was neurologically intact. Oxygen saturation at rest on room air 95%, 93% with exercise.
A complete blood count showed a normal white blood cell count at 6.5 x 109/L (normal, 3.4 – 9.6 x 109/L), with a normal absolute neutrophil count of 3.65 x 109/L (normal, 1.4 – 6.6 x 109/L); the percent distribution of lymphocytes, monocytes, and eosinophils was normal. Her hemoglobin and hematocrit values were 13 gm/dL (normal, 13.2 – 16.6 gm/dL) and 39.7% (normal, 34.9 – 44.5%). The platelet count was normal at 274 x 109/L (normal, 149 – 375 x 109/L). The patient’s serum chemistries and liver function studies were largely normal, including an albumin level at 4.3 gm/dL (normal, 3.5 – 5 gm/dL), with mildly elevated alanine aminotransferase at 59 U/L (normal, 7-45 U/L) and aspartate aminotransferase of 68 U/L (normal, 8-43 U/L); alkaline phosphatase levels, bilirubin, and coagulation studies were normal. SARS-CoV-2 PCR testing was negative. The erythrocyte sedimentation rate was normal at 8 mm/hr (normal, 0-29 mm/hr), as was her C-reactive protein at <2 mg/L (normal, <2 mg/L).
Frontal chest radiography (Figure 1) was performed.
 Figure 1. Frontal and lateral chest radiography. To view Figure 1 in a separate, enlarged window click here.
Figure 1. Frontal and lateral chest radiography. To view Figure 1 in a separate, enlarged window click here.
{kind=link}
Which of the following statements regarding this chest radiograph is accurate? (Click on the correct answer to be directed to the second of seventeen pages)
- Frontal chest radiography shows normal findings
- Frontal chest radiography shows a moderate-to-large right pleural effusion
- Frontal chest radiography shows mediastinal lymphadenopathy
- Frontal chest radiography shows pneumothorax
- Frontal chest radiography shows numerous small nodules
June 2024 Medical Image of the Month: A 76-year-old Man Presenting with Acute Hoarseness
 Figure 1. Anterior-posterior chest x-ray (A) showing moderate elevation of left hemidiaphragm (arrow) and an ill-defined nodular opacity in the left perihilar region (*) suspicious for a hilar mass. Axial image from a contrast enhanced chest CT (B) showing central left upper lobe mass extending into the hilum resulting in narrowing of the vascular and bronchial structures of the left upper lobe.
Figure 1. Anterior-posterior chest x-ray (A) showing moderate elevation of left hemidiaphragm (arrow) and an ill-defined nodular opacity in the left perihilar region (*) suspicious for a hilar mass. Axial image from a contrast enhanced chest CT (B) showing central left upper lobe mass extending into the hilum resulting in narrowing of the vascular and bronchial structures of the left upper lobe.
 Figure 2. 400x magnification hematoxylin and eosin-stained endobronchial biopsy (A) demonstrating malignant cells with large hyperchromatic nuclei (circle) infiltrating through stromal tissue. Compare with the nuclear size of the nearby normal submucosal glands (arrows), 200x magnification image (B) demonstrating poorly differentiated carcinoma cells filling the subepithelial stroma. Normal ciliated mucosal cells are in the upper left of the image (arrowheads).
Figure 2. 400x magnification hematoxylin and eosin-stained endobronchial biopsy (A) demonstrating malignant cells with large hyperchromatic nuclei (circle) infiltrating through stromal tissue. Compare with the nuclear size of the nearby normal submucosal glands (arrows), 200x magnification image (B) demonstrating poorly differentiated carcinoma cells filling the subepithelial stroma. Normal ciliated mucosal cells are in the upper left of the image (arrowheads).
A 76-year-old man with a past medical history significant for coronary artery disease, diabetes mellitus, and 40-pack-year smoking history presented to the emergency department with 1 week of progressive hoarseness. Associated symptoms included a cough initially productive of green sputum that progressed to scant hemoptysis, as well as intermittent hiccups. Four days prior to presentation he sought treatment at a clinic in Mexico, where he was diagnosed with influenza and treated with Tamiflu and Moxifloxacin. His symptoms did not improve, prompting him to seek care at our hospital.
On interview, he denied fevers, chills, dysphagia, otalgia, odynophagia, dyspepsia, chest pain, dyspnea, or weight changes. His temperature was 36.3°C, heart rate 75 beats per minute, blood pressure 150/77 mmHg, respiratory rate 22 breaths per minute, and oxygen saturation 93% on room air. On physical examination, the patient was found to have a hoarse voice, with an otherwise normal oropharyngeal exam. Cardiopulmonary exam was notable for bowel sounds auscultated in the left lower lung fields. The remainder of the exam was unremarkable. Laboratory testing including CBC, CMP, and a respiratory pathogen PCR panel did not detect any viruses.
A chest X-ray was obtained (Figure 1A); imaging was significant for moderate elevation of left hemidiaphragm (A), an ill-defined nodular opacity in the left perihilar region, and suspicion for a hilar mass (B). Chest CT confirmed a large central left upper lobe hilar mass compressing regional vascular and bronchial structures (Figure 1B). The patient underwent Endobronchial ultrasound-guided fine needle aspiration (EBUS FNA) and endobronchial biopsy, which confirmed the diagnosis, recurrent laryngeal nerve injury secondary to left upper lobe non-small cell lung carcinoma (Figure 2).
Hoarseness can be caused by a diverse array of conditions, ranging from local inflammatory processes (e.g., laryngitis or benign vocal cord lesions), to more systemic, neurologic, or oncologic conditions. A systematic evaluation is therefore essential to create an appropriate differential and guide the diagnostic evaluation. This evaluation begins with a detailed history probing for any red flag symptoms: symptoms persisting greater than two weeks, dysphagia, odynophagia, weight loss, or hemoptysis, as was seen in the case above.
Recurrent laryngeal nerve injuries are a less common cause of hoarseness. An understanding of the anatomic course of the recurrent laryngeal nerve (RLN) aids in localizing pathology. The RLN branches off cranial nerve X, also known as the Vagus nerve, and supplies most of the laryngeal muscles. The left RLN extends inferiorly into the chest, and loops posteriorly under the aortic arch before returning superiorly through the neck. Similarly, the right RLN loops posteriorly around the right subclavian artery before traversing superiorly back through the neck. The majority of recurrent laryngeal nerve injuries are iatrogenic, secondary to thyroid or cardiothoracic surgery. However, in the absence of surgery, understanding the anatomy paired with further imaging can help localize the pathology.
The patient’s radiographic findings suggested an intrathoracic mass concerning for a primary lung malignancy. This mass was further characterized on chest CT, which confirmed a large central left upper lobe hilar mass compressing regional vascular and bronchial structures. In the setting of hoarseness, the malignancy was likely causing injury to the recurrent laryngeal nerve. Additionally, given the symptom of hiccups paired with image findings of an elevated hemidiaphragm, the phrenic nerve was also likely being compressed. A biopsy would then further identify the lung mass.
Bronchoscopy showed patent airways and extensive nodular mucosa and endobronchial tumor at the left upper lobe / lingula. Endobronchial biopsy of the left upper lobe revealed infiltrating malignant cells in the submucosal connective tissue. No keratin production or gland formation was seen. Further work-up with immunohistochemical preparations showed the tumor cells to be negative for TTF-1 and p40, markers indicative of pulmonary adenocarcinoma and squamous cell carcinoma, respectively. In light of these features, the most accurate diagnosis is non-small cell carcinoma, not otherwise specified (NOS).
The differential for dysphonia in an adult extends beyond the anatomic boundaries of the laryngopharynx, including an intrathoracic malignancy causing recurrent laryngeal nerve injury. Additionally, phrenic nerve palsy secondary to a mediastinal mass should be included in the differential for an elevated hemidiaphragm.
Alexandra Fuher MD1, Carrie B. Marshall MD2, William Aaron Manning MD3
1Department of Internal Medicine, University of Colorado Anschutz Medical Campus
2Department of Pathology, University of Colorado Anschutz Medical Campus
3Department of Pediatrics, University of Colorado Anschutz Medical Campus
References
- Culp JM, Patel G. Recurrent Laryngeal Nerve Injury. [Updated 2023 May 22]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK560832.
- Reiter R, Hoffmann TK, Pickhard A, Brosch S. Hoarseness-causes and treatments. Dtsch Arztebl Int. 2015 May 8;112(19):329-37. [CrossRef] [PubMed]
- Feierabend RH, Shahram MN. Hoarseness in adults. Am Fam Physician. 2009 Aug 15;80(4):363-70. [PubMed]
- Travis WD, Brambilla E, Noguchi M, et al. Diagnosis of lung cancer in small biopsies and cytology: implications of the 2011 International Association for the Study of Lung Cancer/American Thoracic Society/European Respiratory Society classification. Arch Pathol Lab Med. 2013 May;137(5):668-84. [CrossRef] [PubMed]
September 2023 Medical Image of the Month: Aspergillus Presenting as a Pulmonary Nodule in an Immunocompetent Patient

Figure 1. Chest CT showing 11 x10 mm nodule in the anterior segment of the left upper lobe in the background of emphysematous and basal sub segmental atelectatic changes.
 Figure 2. Lung biopsy low power (A) showing chronic inflammatory infiltrate in the interstitium along with a collection of fungus (arrow) (H&E: x40). Fungus with an area of necrosis (B) (H&E: x100). Numerous thin, narrow-angle, and branching hyphae with septa morphologically consistent with Aspergillus (C) (H&E: x400). Collection of Aspergillus (D). (Periodic acid–Schiff stain: x400).
Figure 2. Lung biopsy low power (A) showing chronic inflammatory infiltrate in the interstitium along with a collection of fungus (arrow) (H&E: x40). Fungus with an area of necrosis (B) (H&E: x100). Numerous thin, narrow-angle, and branching hyphae with septa morphologically consistent with Aspergillus (C) (H&E: x400). Collection of Aspergillus (D). (Periodic acid–Schiff stain: x400).
A 32-year-old nonsmoking woman presented with complaints of recurrent hemoptysis for 5 months and dyspnea on exertion for 1 month. She denied any history of fever, cough, or COVID infection. She has hypothyroidism controlled on thyroxine 25mcg. During the evaluation, she was found to have an enhancing solitary pulmonary nodule (11 x 10 x 9mm) in the anterior segment of the left upper lobe (Figure 1). The patient was given a course of oral antibiotics (amoxicillin /clavulanic acid) and supportive treatment for hemoptysis. Sputum for Ziehl–Neelsen stain and cartridge based nucleic acid amplification test (CBNAAT) was negative. CT- guided biopsy of the nodule was performed. Histopathology showed fungal organisms which were thin, septate with acute angle branching and focal necrotic areas, morphologically consistent with Aspergillus (Figure 2). Serum-specific IgG against aspergillus antigen was normal. The patient was started on oral itraconazole 200mg BID. Follow-up after 1 month showed both symptomatic and radiological improvement. Repeat chest CT showed a significant decrease in size of the nodule.
There is a large spectrum of pulmonary aspergillosis. From this spectrum, pulmonary nodules are a less common manifestation of chronic pulmonary aspergillosis (CPA), especially in immunocompetent individuals. Aspergillus nodules are defined as small, round, discrete, and focal opacities on chest imaging. It can be further classified on basis of internal cavitation (i.e., non-cavitary nodules and cavitary nodules). Differentiating these nodules from other lung pathology may be difficult on CT findings alone and may demand further investigation like image-guided needle aspiration cytology or biopsy, blood investigations like serum Aspergillus precipitin IgG antibody and/or serum Aspergillus galactomannan. Delay in diagnoses may lead to persistence of pulmonary symptoms, and cavitation of the nodule. This entity has a favorable prognosis if managed accordingly. Although there is data regarding surgical management of aspergillus nodules, but data regarding the benefits of anti-fungal therapy in the same is limited.
Diagnosing aspergillus nodules in an immunocompetent individual is a challenge to all pulmonologists. Literature shows limited case reports and small case series on CPA presenting as non-cavitating SPN on radiology. Usually, in such cases, the diagnosis is made following removal or biopsy of the nodule(s), presuming it to be malignant. Patients diagnosed with Aspergillus nodules can’t be differentiated from lung malignant conditions based on demographics, which are usually similar. In the largest case series of Aspergillus nodules done by Muldoon EG et al. (6), 33 patients were reviewed constituting less than 10 % of the cohort of patients with CPA. In a study done by Kang et al. (4) 77% of patients with aspergillus nodules were symptomatic and the most common symptom reported was hemoptysis. Similarly in our case hemoptysis was the chief complaint of the patient. Our patient is a woman and non-smoker similar to previous case reports and series.
In the current guidelines, the detection of serum Aspergillus precipitin IgG antibody is a key diagnostic criterion for CPA. Literature is unclear if the presence of Aspergillus IgG antibody could be considered a supportive finding in the making the diagnosis of Aspergillus nodules. Similarly, in our case also serum specific IgG against Aspergillus fumigatus was negative. Azoles are the primary treatment option in all subtypes of CPA including aspergillus nodule. Our patient also showed disease regression during itraconazole treatment. Another option for management is surgical, though it is associated with significant postoperative complications and recurrence of disease at other sites and must be reserved for selected patients.
Dr. Deependra Kumar Rai, Dr. Priya Sharma, Dr. Vatsal Bhushan Gupta
Department of Pulmonary, Critical Care, and Sleep Medicine
AIIMS Patna, Bihar, India
References
- Kosmidis C, Denning DW. The clinical spectrum of pulmonary aspergillosis. Thorax. 2015 Mar;70(3):270-7. [CrossRef] [PubMed]
- Hansell DM, Bankier AA, MacMahon H, McLoud TC, Müller NL, Remy J. Fleischner Society: glossary of terms for thoracic imaging. Radiology. 2008 Mar;246(3):697-722. [CrossRef] [PubMed]
- Lee SH, Lee BJ, Jung DY, Kim JH, Sohn DS, Shin JW, Kim JY, Park IW, Choi BW. Clinical manifestations and treatment outcomes of pulmonary aspergilloma. Korean J Intern Med. 2004 Mar;19(1):38-42. [CrossRef] [PubMed]
- Kang N, Park J, Jhun BW. Clinical Characteristics and Treatment Outcomes of Pathologically Confirmed Aspergillus Nodules. J Clin Med. 2020 Jul 10;9(7):2185. [CrossRef] [PubMed]
- Yasuda M, Nagashima A, Haro A, Saitoh G. Aspergilloma mimicking a lung cancer. Int J Surg Case Rep. 2013;4(8):690-2. [CrossRef] [PubMed]
- Muldoon EG, Sharman A, Page I, Bishop P, Denning DW. Aspergillus nodules; another presentation of Chronic Pulmonary Aspergillosis. BMC Pulm Med. 2016 Aug 18;16(1):123. [CrossRef] [PubMed]
- Denning DW, Cadranel J, Beigelman-Aubry C, et al. Chronic pulmonary aspergillosis: rationale and clinical guidelines for diagnosis and management. Eur Respir J. 2016 Jan;47(1):45-68. [CrossRef] [PubMed]
- Limper AH, Knox KS, Sarosi GA, et al. An official American Thoracic Society statement: Treatment of fungal infections in adult pulmonary and critical care patients. Am J Respir Crit Care Med. 2011 Jan 1;183(1):96-128. [CrossRef] [PubMed]
- Godet C, Philippe B, Laurent F, Cadranel J. Chronic pulmonary aspergillosis: an update on diagnosis and treatment. Respiration. 2014;88(2):162-74. [CrossRef] [PubMed]
- Kousha M, Tadi R, Soubani AO. Pulmonary aspergillosis: a clinical review. Eur Respir Rev. 2011 Sep 1;20(121):156-74. [CrossRef] [PubMed]
August 2023 Imaging Case of the Month: Chew Your Food Carefully
Michael B Gotway MD1 and Yasmeen M Butt MD2
1Departments of Radiology and 2Laboratory Medicine, Division of Anatomic Pathology
Mayo Clinic-Arizona
Scottsdale, Arizona USA
History of Present Illness
A 50-year-old woman presents with a history of chronic dyspnea and cough, becoming particularly problematic following COVID-19 infection 4 months prior to presentation. While she did experience significant periodic oxygen desaturations during her COVID-19 infection, she was not hospitalized for this illness. The patient also reported wheezing in the previous few weeks.
Past Medical History, Family History and Social History
The patient’s past medical history was also notable for gastroesophageal reflux disease as well as both Coombs positive and iron deficiency anemia. She reports a history of asthma, well controlled with inhaler use.
The patient’s past surgical history included adenoidectomy, cholecystectomy, and gastric laparoscopic band placement.
Her medications included prednisone (20 mg daily), dextroamphetamine-amphetamine, furosemide, omeprazole, fluoxetine, zolpidem (Ambien), daily Bactrim, occasional Loratadine (Claritin). She also utilized an albuterol inhaler and Fluticasone-based (both Flonase and Breo Ellipta) inhalers.
The patient is a former smoker, ½ pack-per day for 26 years, having quit 11 years prior to presentation. She also reported a history of vaping (agent inhaled unclear) for 8 years, quitting 3 years earlier. She has no known allergies. She drinks alcohol socially and denied illicit drug use.
Physical Examination
The patient’s physical examination showed her temperature to be 99°F with normal pulse and respiratory rate but her blood pressure elevated at 160/90 mmHg. She was obese (263 lbs., BMI= 41). Bilateral basal rales were noted at her examination, but no other abnormal physical examination findings were detected.
Laboratory Evaluation
The patient’s room air pulse oximetry was 85%. A complete blood count showed an upper normal white blood cell count at 1.9 x109/L (normal, 4.5 – 11 x109/L). Her hemoglobin and hematocrit values were 10.7 gm/dL (normal, 12 – 16 gm/dL) and 37.1% (normal, 36 – 46%). The patient’s serum chemistries and liver function studies were entirely normal. The patient had an elevated anti-nuclear antibody titer at 1:320. An echocardiogram noted diastolic dysfunction but normal left ventricular contractility.
Frontal chest radiography (Figure 1) was performed.

Figure 1. Frontal chest radiography.
Which of the following statements regarding this chest radiograph is accurate? (Click on the correct answer to be directed to the second of 11 pages)
- Frontal chest radiography shows normal findings
- Frontal chest radiography shows marked cardiomegaly
- Frontal chest radiography shows mediastinal lymphadenopathy
- Frontal chest radiography shows pleural effusion
- Frontal chest radiography shows multifocal peribronchial consolidation
June 2023 Medical Image of the Month: Solitary Fibrous Tumor of the Pleura
 Figure 1. Posterior to anterior ultrasound image of the lower left hemithorax (A) captured during a therapeutic left-sided thoracentesis. There is a bilobed pedunculated mass (*) attached to the left lower lobe which was not noticed at the time of the procedure, but was identified in retrospect after the mass was discovered on CT. Sagittal reconstruction (B) from a 17-FDG PET-CT also demonstrate the bilobed left lower lobe mass (*). The mass demonstrates diffuse low-level FDG update suggesting relatively low metabolic activity. The appearance of the mass is very similar compared to the image capture from the thoracentesis.
Figure 1. Posterior to anterior ultrasound image of the lower left hemithorax (A) captured during a therapeutic left-sided thoracentesis. There is a bilobed pedunculated mass (*) attached to the left lower lobe which was not noticed at the time of the procedure, but was identified in retrospect after the mass was discovered on CT. Sagittal reconstruction (B) from a 17-FDG PET-CT also demonstrate the bilobed left lower lobe mass (*). The mass demonstrates diffuse low-level FDG update suggesting relatively low metabolic activity. The appearance of the mass is very similar compared to the image capture from the thoracentesis.
 Figure 2. Axial (A) and sagittal oblique (B) reconstructions from a contrast-enhanced chest CT demonstrates a large, heterogeneously enhancing bilobed mass (*) arising from, and connected to the posterior left lower lobe via a small vascular pedicle (arrow).
Figure 2. Axial (A) and sagittal oblique (B) reconstructions from a contrast-enhanced chest CT demonstrates a large, heterogeneously enhancing bilobed mass (*) arising from, and connected to the posterior left lower lobe via a small vascular pedicle (arrow).
 Figure 3. High-powered H & E stain (A) from surgical pathology specimen demonstrates a haphazard arrangement of spindled and ovoid cells with relatively featureless architecture. Other slides demonstrated variable myxoid stroma and areas of dilated, branching “staghorn” vessels. The cells stain strongly positive for CD34 (B) consistent with solitary fibrous tumor of the pleura.
Figure 3. High-powered H & E stain (A) from surgical pathology specimen demonstrates a haphazard arrangement of spindled and ovoid cells with relatively featureless architecture. Other slides demonstrated variable myxoid stroma and areas of dilated, branching “staghorn” vessels. The cells stain strongly positive for CD34 (B) consistent with solitary fibrous tumor of the pleura.
An 85-year-old man presented to our institution for a second opinion and for management of a recurrent left-sided pleural effusion. The patient has a history of CLL, which was diagnosed with a chest wall biopsy 4 years prior to presentation. Since that time, he has undergone chemotherapy and had a good response. In the past 18 months, the patient has had their left-sided pleural effusion drained 24 times. The patient also has a history of hypothyroidism and has had a cholecystectomy.
The patient brought multiple outside imaging studies with him for review. An image capture from a recent ultrasound-guided left thoracentesis (Figure 1A) demonstrated, in retrospect, a pedunculated left lower lobe mass. An outside PET-CT (Figure 1B) was also available, confirming the presence of this mass, which had relatively uniform, low level FDG uptake such that it evade notice on first interpretation. A CT angiogram (Figure 2) demonstrated a large, bilobed mass with heterogeneous arterial enhancement that was attached to and arising from the visceral pleura of the left lower lobe. The angiographic scanning phase demonstrated a well-developed vascular pedicle by which the mass attached to the left lower lobe. Needle biopsy (and subsequent resection) of the mass revealed a 13.5 cm solidary fibrous tumor of the pleura.
Solitary fibrous tumor of the pleura (SFTP) was first described by Klemperer and Rabin in 1931 and has undergone multiple name changes over the years, having been called benign mesothelioma, localized mesothelioma, solitary fibrous mesothelioma, pleural fibroma, submesothelial fibroma, subserosal fibroma, and localized fibrous tumor at various points in the past (1). SFTP is a rare tumor, accounting for less than 5% of tumors arising from the pleura (2). Although it can rarely arise outside the pleura (peritoneum, pericardium, meninges), it most commonly arises from the pleura. It can arise from either the visceral or parietal pleural layer and tends to have a pedunculated attachment in the case of the former with a more broad-based attachment in the case of the later (3). In the case of a SFTP arising from the visceral pleura, it’s pedunculated nature may result in a “wandering” chest mass (4).
SFTP most commonly presents incidentally, often on an imaging study. Imaging findings can be relatively nonspecific, aside from pleural origin. Probably the most salient lesson from this case is to be sure to be sure to perform a diagnostic analysis of any imaging obtained for procedural guidance. SFTP’s are probably best known for the two unusual clinical syndromes that have been described in association with them. There may be hypertrophic pulmonary osteoarthropathy (Pierre-Marie-Bamberg syndrome), which is caused by osteolysis related to the excessive release of hyaluronic acid. There may also refractory hypoglycemia (Doege-Potter syndrome), which is caused by release of insulin-like growth factor II by the tumor cells (4).
Clinton Jokerst MD, Matthew Stib MD, Carlos Rojas MD, Kristopher Cummings MD, Eric Jensen MD, Prasad Panse MD, and Michael Gotway MD
Department of Radiology, Mayo Clinic Arizona, Scottsdale, AZ USA
References
- Klemperer P, Rabin CB. Primary neoplasm of the pleura: a report of five cases. Arch Pathol. 1931;11:385-412.
- Shields TW. Localized fibrous tumors of the pleura. In: Shields TW, ed. General Thoracic Surgery. 4th ed. Baltimore, Md: Williams & Wilkins; 1994
- Robinson LA. Solitary fibrous tumor of the pleura. Cancer Control. 2006 Oct;13(4):264-9. [CrossRef] [PubMed]
- Bhardwaj H, Lindley S, Bhardwaj B, Carlile PV, Huard DR. Catch me if you can: a wandering solitary fibrous tumor of the pleura. Am J Respir Crit Care Med. 2014 Aug 1;190(3):e7-9. [CrossRef] [PubMed]
- Luciano C, Francesco A, Giovanni V, Federica S, Cesare F. CT signs, patterns and differential diagnosis of solitary fibrous tumors of the pleura. J Thorac Dis. 2010 Mar;2(1):21-5. [PubMed]
July 2022 Medical Image of the Month: Pulmonary Nodule in the Setting of Pyoderma Gangrenosum (PG)

Figure 1. Unenhanced lung window chest CT images in the axial (A) and sagittal (B) planes show a solid, non-calcified irregular left upper lobe mass (arrow) with spiculated margins. The nodule demonstrates enhancement on soft tissue windows (C) with associated mediastinal adenopathy (arrowhead). The mass and adenopathy are FDG-avid on axial fused PET-CT image (D).

Figure 2. (A) Photograph of one of the patient’s skin lesions. (B) Hematoxylin and Eosin stained low-power pathological image of a biopsy specimen from a skin lesion demonstrates dense mixed neutrophilic dermal inflammation. Extensive infectious and neoplastic workup was negative. The histopathologic diagnosis was consistent with pyoderma gangrenosum.
A 70-year-old man presented with persistent cough productive of clear sputum which had persisted approximately 12 months after COVID-19 infection. The patient reported a more recent history of night sweats and had also recently developed what he described as “blisters” on his chest wall and right shoulder starting 4 weeks prior to presentation that “opened up” giving off a bloody discharge. The patient had been treated with trimethoprim-sulfamethoxazole and doxycycline without improvement and reported a 10-pound weight loss over the past several months. The patient was a never-smoker with no significant travel history and a past medical history of asthma, GERD, gout, and chronic rhinitis. He had no history of autoimmune/inflammatory diseases or malignancy.
Vital signs and physical exam were normal, except for a 1 cm open wound in the center of the patient’s chest [Figure 2A]. A chest CT performed as part of the patient’s workup demonstrated a spiculated mass in the left upper lobe with adjacent mediastinal adenopathy [Figure 1A-C]. This prompted an FDG PET-CT, which demonstrated some increased uptake in the mass and adjacent lymph nodes [Figure 1D]. The mass was biopsied via bronchoscopy, pathology was nondiagnostic with rare groups of benign-appearing bronchial epithelial cells and blood. The skin lesion was biopsied next demonstrating dense mixed neutrophilic dermal inflammation [Figure 2B]. The diagnosis of pyoderma gangrenosum was made and the patient was treated with NSAIDs and a systemic glucocorticoid (40 mg/day, tapered over 10 weeks).steroid taper, The pulmonary mass , mediastinal lymph nodes and skin lesions all resolved over time.
Pyoderma gangrenous (PG) is a misnomer in every sense as it is neither infectious nor gangrenous. It is a rare (3-10 cases/million/year) disorder of skin characterized by neutrophilic dermatosis which usually presents as a with inflammatory and ulcerative disorder of the skin lesions and is usually a diagnosis of exclusion (1). PG has no pathognomonic clinical or histological findings. Majority of the cases have an underlying systemic disease, commonly inflammatory bowel disease (41%), inflammatory arthritis (20.5%) and oncologic or hematologic disorders (17.2%). While it can in any age group including children, the peak age of onset is 40-60 years. There is a slight female preponderance (2). The most common presentation is inflammatory papule or pustule that progress to a painful ulcer with violaceous undermined borders and a purulent base. The lesions commonly occur in surgical wounds within 2 weeks of surgery, a phenomenon known as pathergy, and often lead to wound dehiscence (3). The lesions may also be peristomal in patients with IBD. Extracutaneous lesions have been reported in liver, intestine, spleen, cornea, bones, muscles, CNS and rarely, in the lungs (4-6).
There have been <50 cases of pulmonary PG ever described in literature (7,8). The patients may present with non-specific symptoms of cough, dyspnea, fever, weight-loss, malaise and occasionally hemoptysis. Chest imaging may show cavitary infiltrates. The diagnosis is established by cutaneous or extracutaneous lesion biopsy of the ulcer edge showing neutrophilic infiltrate. Extensive testing should be performed , extensive testing to rule out alternative causes including infection, and malignancy, in setting of underlying inflammatory bowel disease or inflammatory arthritisautoimmune and inflammatory conditions associated with PG. Presence of pathergy and response to anti-inflammatory therapy also support the diagnosis (9). Treatment includes systemic or intralesional glucocorticoids and/or calcineurin inhibitors (3). Use of TNF alpha inhibitor, infliximab and anti-neutrophil antimicrobial dapsone has also been described in case reports (10). Most patients achieve remission within 6 months to 3 years.
Umesh Goswami MD1, Michael Gotway MD2, Carlos Rojas MD2, Prasad Panse MD2, Kris Cummings MD2, Eric Jensen MD2, Kenneth Sakata, MD1 and Clinton Jokerst MD2
Division of Pulmonology1 and Department of Radiology2
Mayo Clinic Arizona, Scottsdale, AZ USA
References
- Ruocco E, Sangiuliano S, Gravina AG, Miranda A, Nicoletti G. Pyoderma gangrenosum: an updated review. J Eur Acad Dermatol Venereol. 2009 Sep;23(9):1008-17. [CrossRef] [PubMed]
- Ashchyan HJ, Butler DC, Nelson CA, et al. The Association of Age With Clinical Presentation and Comorbidities of Pyoderma Gangrenosum. JAMA Dermatol. 2018 Apr 1;154(4):409-413. [CrossRef] [PubMed]
- Binus AM, Qureshi AA, Li VW, Winterfield LS. Pyoderma gangrenosum: a retrospective review of patient characteristics, comorbidities and therapy in 103 patients. Br J Dermatol. 2011 Dec;165(6):1244-50. [CrossRef] [PubMed]
- Vadillo M, Jucgla A, Podzamczer D, Rufi G, Domingo A. Pyoderma gangrenosum with liver, spleen and bone involvement in a patient with chronic myelomonocytic leukaemia. Br J Dermatol. 1999 Sep;141(3):541-3. [CrossRef] [PubMed]
- Scherlinger M, Guillet S, Doutre MS, Beylot-Barry M, Pham-Ledard A. Pyoderma gangrenosum with extensive pulmonary involvement. J Eur Acad Dermatol Venereol. 2017 Apr;31(4):e214-e216. [CrossRef] [PubMed]
- Abdelrazeq AS, Lund JN, Leveson SH. Pouchitis-associated pyoderma gangrenosum following restorative proctocolectomy for ulcerative colitis. Eur J Gastroenterol Hepatol. 2004 Oct;16(10):1057-8. [CrossRef] [PubMed]
- Gade M, Studstrup F, Andersen AK, Hilberg O, Fogh C, Bendstrup E. Pulmonary manifestations of pyoderma gangrenosum: 2 cases and a review of the literature. Respir Med. 2015 Apr;109(4):443-50. [CrossRef] [PubMed]
- Sakata KK, Penupolu S, Colby TV, Gotway MB, Wesselius LJ. Pulmonary pyoderma gangrenosum without cutaneous manifestations. Clin Respir J. 2016 Jul;10(4):508-11. [CrossRef] [PubMed]
- Maverakis E, Ma C, Shinkai K, et al. Diagnostic Criteria of Ulcerative Pyoderma Gangrenosum: A Delphi Consensus of International Experts. JAMA Dermatol. 2018 Apr 1;154(4):461-466. [CrossRef] [PubMed]
- Teasley LA, Foster CS, Baltatzis S. Sclerokeratitis and facial skin lesions: a case report of pyoderma gangrenosum and its response to dapsone therapy. Cornea. 2007 Feb;26(2):215-9. [CrossRef] [PubMed]
Cite as: Goswami U, Gotway M, Rojas C, Panse P, Cummings K, Jensen E, Sakata K, Jokerst C. July 2022 Medical Image of the Month: Pulmonary Nodule in the Setting of Pyoderma Gangrenosum (PG). Southwest J Pulm Crit Care Sleep. 2022:25(1):4-6. doi: https://doi.org/10.13175/swjpccs029-22 PDF
March 2022 Medical Image of the Month: Pulmonary Nodules in the Setting of Diffuse Idiopathic Pulmonary NeuroEndocrine Cell Hyperplasia (DIPNECH)

Figure 1. Unenhanced chest CT images in the axial plane show solid, non-calcified and well-circumscribed nodules in the right upper lobe (RUL) (A) and lingula (B). The RUL nodule is FDG-avid on axial fused FDG PET-CT image (C) whereas the lingular nodule is not (D).

Figure 2. Unenhanced chest CT images in the axial plane reconstructed with maximum intensity projection (MIP, A) and minimum intensity projection (MinIP, B) techniques show multiple scattered solid pulmonary nodules (arrows) and pulmonary mosaicism consistent with air-trapping (circled). Axial fused images from a 68GA-DOTATATE PET-CT demonstrate some activity in the RUL nodule (C) and more prominent uptake in the lingular nodule (D).

Figure 3. Hematoxylin and Eosin stained low-power pathological image (A) demonstrates the lingular carcinoid tumor (*) as well as several carcinoid tumorlets (arrows) in the adjacent lung. A separate specimen of lung stained with synaptophysin demonstrates multiple tumorlets in the small sample. When taken in conjunction with imaging findings, pathology is in-keeping with a diagnosis of Diffuse Idiopathic Pulmonary Neuroendocrine Cell Hyperplasia (DIPNECH).
A 62-year-old woman presented to an outside hospital with chronic cough, prompting a chest x-ray (CXR). Findings further prompted unenhanced chest CT to evaluate possible pulmonary nodules. The CT demonstrated multiple scattered, solid and centrilobular pulmonary nodules, most of which were small but there were two >1 cm nodules, one in the right upper lobe (RUL) and a second in the lingula (Figure 1A,B). A subsequent FDG PET-CT was performed demonstrating increased metabolic activity in the RUL nodule with no activity in the lingular nodule (Figure 1C,D). Biopsy of the RUL nodule was consistent with a carcinoid. At this point the patient was referred to our center for further management. A repeat chest CT failed to demonstrate any significant change in the nodules. MIP and MinIP reconstructions from that examination demonstrate multiple small, solid pulmonary nodules (arrows) (Figure 2A), many of which were associated with air-trapping resulting in pulmonary mosaicism (circled) (Figure 2B). A 68GA-DOTATATE PET-CT was performed, the results of which provide stark contrast to the FDG-PET in that the RUL nodule demonstrated modest uptake (Figure 2C), whereas the lingular nodule showed very prominent update (Figure 2D). The lingular nodule was resected, H & E-stained pathology image (Figure 3A) demonstrated a typical carcinoid (*) with multiple carcinoid tumorlets in the surgical specimen (arrows). A separate specimen stained with synaptophysin demonstrates multiple neuroendocrine tumorlets. Pathological findings, in conjunction with patient demographics and imaging findings, were consistent with Diffuse Idiopathic Pulmonary NeuroEndocrine Cell Hyperplasia (DIPNECH).
DIPNECH is recognized as a pre-neoplastic lesion in the 2015 WHO classification of lung tumors (1). There is neuroendocrine cell proliferation within the small bronchi and bronchioles which may progress beyond the basement membrane, forming carcinoid tumorlets and in some cases, eventually carcinoid tumors. These airway-centered nodules cause obstruction. In addition, there is often an association between DIPNECH and constrictive bronchiolitis, which causes further airway obstruction (2). The vast majority of patients are women in their 50s-70s and most patients are symptomatic with the most common presenting symptoms being chronic cough and dyspnea (3,4). Many of these patients are often mis-diagnosed with asthma initially (4). The imaging findings of DIPNECH on CT are not specific but can be pathognomonic in some cases. There are almost always innumerable small solid (and sometimes ground glass) centrilobular nodules and nodular bronchial thickening with associated pulmonary mosaicism related to air trapping. Nodules are either stable or very slowly growing over years with the largest nodules usually being biopsied or resected and yielding typical carcinoid on pathology (4). A relatively new nuclear medicine imaging study, 68Ga-DOTATATE PET-CT, shows promise as a higher resolution and more sensitive examination for detection of neuroendocrine tumors (relative to octreotide scans), including pulmonary carcinoid tumors in the setting of DIPNECH (5,6).
Clinton Jokerst MD1, Henry Tazelaar2, Carlos Rojas MD1, Prasad Panse MD1, Kris Cummings MD1, Eric Jensen MD1 and Michael Gotway MD1
Departments of Radiology1 and Pathology2
Mayo Clinic Arizona, Scottsdale, AZ USA
References
- Gosney JR, Austin JHM, Jett J, et al. Diffuse pulmonary neuroendocrine cell hyperplasia. In: Travis WD, Brambilla E, Burke AP, et al., eds. WHO classification of tumours of the lung, pleura, thymus and heart. Lyon, IARC Press, 2015; pp. 78-79.
- Samhouri BF, Azadeh N, Halfdanarson TR, Yi ES, Ryu JH. Constrictive bronchiolitis in diffuse idiopathic pulmonary neuroendocrine cell hyperplasia. ERJ Open Res. 2020 Nov 16;6(4):00527-2020. [CrossRef] [PubMed]
- Rossi G, Cavazza A, Spagnolo P, Sverzellati N, Longo L, Jukna A, Montanari G, Carbonelli C, Vincenzi G, Bogina G, Franco R, Tiseo M, Cottin V, Colby TV. Diffuse idiopathic pulmonary neuroendocrine cell hyperplasia syndrome. Eur Respir J. 2016 Jun;47(6):1829-41. [CrossRef] [PubMed]
- Little BP, Junn JC, Zheng KS, Sanchez FW, Henry TS, Veeraraghavan S, Berkowitz EA. Diffuse Idiopathic Pulmonary Neuroendocrine Cell Hyperplasia: Imaging and Clinical Features of a Frequently Delayed Diagnosis. AJR Am J Roentgenol. 2020 Dec;215(6):1312-1320. [CrossRef] [PubMed]
- Deppen SA, Blume J, Bobbey AJ, Shah C, Graham MM, Lee P, Delbeke D, Walker RC. 68Ga-DOTATATE Compared with 111In-DTPA-Octreotide and Conventional Imaging for Pulmonary and Gastroenteropancreatic Neuroendocrine Tumors: A Systematic Review and Meta-Analysis. J Nucl Med. 2016 Jun;57(6):872-8. [CrossRef] [PubMed]
- Fraum TJ, Ritter JH, Chen DL. Diffuse Idiopathic Pulmonary Neuroendocrine Cell Hyperplasia on Somatostatin Receptor Imaging. Am J Respir Crit Care Med. 2018 Nov 1;198(9):1223-1225. [CrossRef] [PubMed]
Cite as: Jokerst C, Tazelaar H, Rojas C, Panse P, Cummings K, Jensen E, Gotway M. March 2022 Medical Image of the Month: Pulmonary Nodules in the Setting of Diffuse Idiopathic Pulmonary Neuroendocrine Cell Hyperplasia (DIPNECH). Southwest J Pulm Crit Care Sleep;2022:40-42. doi: https://doi.org/10.13175/swjpccs010-22 PDF
Medical Image of the Month: Metastatic Pulmonary Calcifications in a Kidney Transplant Recipient

Figure 1. Axial and coronal views of thoracic CT scan showing upper lobe predominant centrilobular ground glass nodules.

Figure 2. Transbronchial biopsy yielded nine tissue fragments, each of which demonstrated moderate to marked interstitial calcification (amorphous purple material) along the alveolar septae, perivascular spaces and within the bronchioles consistent metastatic calcification. There were secondary changes of mild alveolar fibrosis and interstitial hemosiderin laden macrophages (golden brown pigment). There was no evidence of an inflammatory response or malignancy to otherwise explain the CT findings in this patient.
A 40-year-old man presented with shortness of breath, cough and abnormal imaging. He had a past medical history of end stage renal disease (ESRD) secondary to Alport syndrome and underwent three kidney transplants in 2004, 2010 and 2016. He was intermittently on dialysis between the transplants. He also had a history of coronary artery disease, congestive heart failure and parathyroidectomy. His CT scan (Figure 1) from 2019 showed diffuse centrilobular ground glass opacities sparing the peripheral lung and lung bases. Pulmonary function testing showed obstruction, with reduced diffusion capacity. Bronchoscopy with bronchoalveloar lavage and transbronchial biopsy of the right upper and middle lobes was consistent with metastatic pulmonary calcification (MPC) (Figure 2).
MPC is a rare metabolic pulmonary disease which is usually found incidentally or on autopsy. It occurs with chronically elevated calcium and phosphorus levels (1). It is very commonly associated with ESRD and rarely in primary hyperparathyroidism, osteoporosis, sarcoidosis, renal and liver transplant and hematological malignancies (2-5). CT shows diffuse, nodular areas of ground-glass opacity or consolidation seen in the upper lung zones with pleural sparing. Diagnosis is made on histopathology. There is no definitive treatment for MPC. MPC should be considered with radiological nodular ground glass opacities, particularly in the context of chronic kidney disease or kidney transplant.
Nikhil Madan1 MD FCCP, Vipul Patel1 MD, Christine Minerowicz2 MD, Harpreet Greewal1 MD, and Thomas Kaleekal MD FCCP
1Division of Pulmonary and Critical Care and Transplant
Newark Beth Israel Medical Center
Newark, NJ USA
2Department of Pathology and Laboratory Medicine
Rutgers Robert Wood Johnson Medical School
New Brunswick, NJ USA
References
-
Chan ED, Morales DV, Welsh CH, McDermott MT, Schwarz MI. Calcium deposition with or without bone formation in the lung. Am J Respir Crit Care Med. 2002 Jun 15;165(12):1654-69. [CrossRef] [PubMed]
-
Kuhlman JE, Ren H, Hutchins GM, Fishman EK. Fulminant pulmonary calcification complicating renal transplantation: CT demonstration. Radiology. 1989; 173:459e60. [CrossRef] [PubMed]
-
Bendayan D, Barziv Y, Kramer MR. Pulmonary calcifications: a review. Respir Med. 2000; 94:190e3. [CrossRef] [PubMed]
-
Izadyar M, Mahjoub F, Ardakani SN, Ahmadi J. Pulmonary metastatic calcification in a leukemic patient: a case report. J Pediatr Hematol Oncol. 2010;32:e108e10. [CrossRef] [PubMed]
-
Surani SR, Surani S, Khimani A, Varon J. Metastatic pulmonary calcification in multiple myeloma in a 45-year-old man. Case Reports Pulmonol. 2013; 2013:341872. [CrossRef] [PubMed]
Cite as: Madan N, Patel V, Minerowicz C, Greewal H, Kaleekal T. Medical image of the month: metastatic pulmonary calcifications in a kidney transplant recipient. Southwest J Pulm Crit Care. 2020;20(2):71-2. doi: https://doi.org/10.13175/swjpcc001-20 PDF
Medical Image of the Week: Tracheobronchopathia Osteochondroplastica

Figure 1. View of trachea during bronchoscopy showing submucosal nodules.

Figure 2. H & E staining of cartilage biopsy.
A 52-year-old asymptomatic woman underwent a low dose computed tomography (CT) of chest due to long-standing history of smoking. CT chest revealed a 4 mm right lower lobe pulmonary nodule. Also noted were several nodules throughout the trachea and in the left main-stem bronchus. Bronchoscopy revealed multiple non-obstructing submucosal nodules along the tracheal rings with sparing of the posterior membranous portion of the trachea (Figure 1). Endotracheal biopsy showed benign cartilage and ciliated epithelium (Figure 2). The patient was diagnosed with tracheobronchopathia osteochondroplastica (TO). Clinical manifestations of TO are nonspecific and include cough, wheezing, hemoptysis, dyspnea, and recurrent lung infections (1). Therapy for TO includes alleviation of symptoms with bronchodilators, treatment of respiratory infections and tracheal dilation. Therapeutic modalities for tracheal dilation includes surgical resection, laser ablation and vaporization. CT chest was to be repeated at 12 months for follow-up of the pulmonary nodule. The patient was lost to follow-up.
Benjamin O. Lawson MD1, Kelechi Abarikwu2, and Aditya Gupta MD3
1Internal Medicine and 3Pulmonary/Critical Care Medicine
HonorHealth Scottsdale Thompson Peak Medical Center
Scottsdale, AZ USA
2University of Arizona Tucson
Tucson, AZ USA
Reference
- Simmons C, Vinh D, Donovan DT, Ongkasuwan J. Tracheobronchopathia osteochondroplastica. Laryngoscope. 2016 Sep;126(9):2006-9. [CrossRef] [PubMed]
Cite as: Lawson BO, Abarikwu K, Gupta A. Medical image of the week: Tracheobronchopathia osteochondroplastica. Southwest J Pulm Crit Care. 2018;17(2):45-6. doi: https://doi.org/10.13175/swjpcc094-18 PDF
August 2017 Imaging Case of the Month
Brandon T. Larsen, MD, PhD1
Michael B. Gotway, MD2
Departments of Pathology1 and Radiology2
Mayo Clinic Arizona
Scottsdale, Arizona USA
Clinical History: A 67-year-old man with a 23 pack-year history of smoking, stopping 6 years earlier, presented with a year-long history of intermittent hemoptysis consisting of small specs of blood particularly in the morning after he awoke. No sputum discoloration was reported and the patient denied shortness of breath, fever, shortness of breath, and chills. The patient also denied rash, joint pain, and night sweats. His past surgical history was remarkable only for an appendectomy, tonsillectomy, and repair of an ankle fracture, all as a young man. The patient did report some asbestos exposure in the past. He takes a multivitamin and occasional over-the counter pain relievers, but was not taking prescription medications.
Physical examination: unremarkable and the patient’s oxygen saturation was 98% on room air.
Laboratory evaluation: largely unremarkable. Quantiferon testing for Mycobacterium tuberculosis was negative. An outside otolaryngology examination was reported to show no abnormalities. Frontal chest radiography (Figure 1) was performed.

Figure 1. Frontal chest radiography.
Which of the following statements regarding the chest radiograph is most accurate? (Click on the correct answer to proceed to the second of nine pages)
- The chest radiograph shows a mediastinal mass
- The chest radiograph shows multifocal consolidation and pleural effusion
- The chest radiograph shows multifocal smooth interlobular septal thickening
- The chest radiograph shows a possible focal air space opacity
- The chest radiograph shows small cavitary pulmonary nodules
Cite as: Larsen BT, Gotway MB. August 2017 imaging case of the month. Southwest J Pulm Crit Care. 2017;15(2):69-79. doi: https://doi.org/10.13175/swjpcc098-17 PDF
March 2017 Imaging Case of the Month
Courtney M. Tomblinson, MD and Michael B. Gotway, MD
Department of Radiology
Mayo Clinic Arizona
Scottsdale, Arizona USA
Clinical History: A 69-year-old man presented with long-standing complaints of dyspnea, progressing to dyspnea at rest, associated with some dysphagia to solids. He also noted symptoms consistent with exertional stertor (a respiratory sound characterized by heavy snoring or gasping). His past medical history was remarkable only for hypertension controlled with medication.
Laboratory data, include white blood cell count, coagulation profile, and serum chemistries were within normal limits. Oxygen saturation on room air was normal.
Frontal chest radiography (Figure 1) was performed.

Figure 1: Frontal chest radiography.
Which of the following statements regarding the chest radiograph is most accurate? (Click on the correct answer to proceed to the second of nine pages)
- Frontal chest radiography shows a cavitary lung mass
- Frontal chest radiography shows an abnormal mediastinal contour
- Frontal chest radiography shows multiple small nodules
- Frontal chest radiography shows peribronchial and mediastinal lymphadenopathy
- Frontal chest radiography shows pleural effusion
Cite as: Tomblinson CM, Gotway MB. March 2017 imaging case of the month. Southwest J Pulm Crit Care. 2017;14(3):104-16. doi: https://doi.org/10.13175/swjpcc029-17 PDF
March 2016 Imaging Case of the Month
Michael B. Gotway, MD
Department of Radiology
Mayo Clinic Arizona
Scottsdale, AZ USA
Imaging Case of the Month CME Information
Members of the Arizona, New Mexico, Colorado and California Thoracic Societies and the Mayo Clinic are able to receive 0.25 AMA PRA Category 1 Credits™. Completion of an evaluation form is required to receive credit and a link is provided on the last panel of the activity.
0.25 AMA PRA Category 1 Credit(s)™
Estimated time to complete this activity: 0.25 hours
Lead Author(s): Michael B. Gotway, MD. All Faculty, CME Planning Committee Members, and the CME Office Reviewers have disclosed that they do not have any relevant financial relationships with commercial interests that would constitute a conflict of interest concerning this CME activity.
Learning Objectives:
As a result of this activity I will be better able to:
- Correctly interpret and identify clinical practices supported by the highest quality available evidence.
- Will be better able to establsh the optimal evaluation leading to a correct diagnosis for patients with pulmonary, critical care and sleep disorders.
- Will improve the translation of the most current clinical information into the delivery of high quality care for patients.
- Will integrate new treatment options in discussing available treatment alternatives for patients with pulmonary, critical care and sleep related disorders.
Learning Format: Case-based, interactive online course, including mandatory assessment questions (number of questions varies by case). Please also read the Technical Requirements.
CME Sponsor: University of Arizona College of Medicine at the Arizona Health Sciences Center.
Current Approval Period: January 1, 2015-December 31, 2016
Financial Support Received: None.
Clinical History: A 66 year-old man with orthotopic heart transplantation 1 year previously presented with complaints of recent-onset small volume (<1 teaspoon) hemoptysis, post-nasal drip, and night sweats. The patient indicated he had recent contact with several young grandchildren who had upper respiratory tract symptoms. The patient’s past medical history was remarkable for recurrent constrictive pericarditis (surgically treated), hypertension, type II diabetes mellitus (treated with insulin), psoriasis, sleep-disordered breathing, and grade 2 cardiac transplant rejection diagnosed 6 months earlier. The patient’s medication list included insulin, Cellcept (mycophenolate mofetil), Prograf (tacrolimus), prednisone, among others. On physical examination, the patient was mildly tachycardic (heart rate = 104 beats/minute) with an oxygen saturation on room air of 92%. The white blood cell count was within the normal range, but C-reactive protein and B-type natriuretic peptide levels were reportedly elevated.
Frontal chest radiography (Figure 1) was performed, with a radiograph from one month other also shown for comparison.

Figure 1. Frontal (A) chest radiography shows interval development of a thick-walled left lower lobe cavity since a chest radiograph performed one month previously.
Which of the following statements regarding the chest radiograph is most accurate? (Click on the correct answer to proceed to the second of eight panels)
Cite as: Gotway MB. March 2016 imaging case of the month. Southwest J Pulm Crit Care. 2016(Mar);12(3):90-101. doi: http://dx.doi.org/10.13175/swjpcc023-16 PDF
February 2016 Imaging Case of the Month
Michael B. Gotway, MD
Department of Radiology
Mayo Clinic Arizona
Scottsdale, AZ
Imaging Case of the Month CME Information
Members of the Arizona, New Mexico, Colorado and California Thoracic Societies and the Mayo Clinic are able to receive 0.25 AMA PRA Category 1 Credits™. Completion of an evaluation form is required to receive credit and a link is provided on the last panel of the activity.
0.25 AMA PRA Category 1 Credit(s)™
Estimated time to complete this activity: 0.25 hours
Lead Author(s): Michael B. Gotway, MD. All Faculty, CME Planning Committee Members, and the CME Office Reviewers have disclosed that they do not have any relevant financial relationships with commercial interests that would constitute a conflict of interest concerning this CME activity.
Learning Objectives:
As a result of this activity I will be better able to:
- Correctly interpret and identify clinical practices supported by the highest quality available evidence.
- Will be better able to establsh the optimal evaluation leading to a correct diagnosis for patients with pulmonary, critical care and sleep disorders.
- Will improve the translation of the most current clinical information into the delivery of high quality care for patients.
- Will integrate new treatment options in discussing available treatment alternatives for patients with pulmonary, critical care and sleep related disorders.
Learning Format: Case-based, interactive online course, including mandatory assessment questions (number of questions varies by case). Please also read the Technical Requirements.
CME Sponsor: University of Arizona College of Medicine at the Arizona Health Sciences Center.
Current Approval Period: January 1, 2015-December 31, 2016
Financial Support Received: None.
Clinical History: A 78 year-old woman presented to her physician for routine care. Her past medical history included hyperlipidemia, hypothyroidism, gout, hypertension, and arthritis.
Although she was asymptomatic, screening frontal and lateral chest radiography (Figure 1) was performed.

Figure 1. Frontal (A) and lateral (B) chest radiography.
Which of the following statements regarding the chest radiograph is most accurate? (Click on the correct answer to proceed to the second of nine panels)
Cite as: Gotway MB. February 2016 imaging case of the month. Southwest J Pulm Crit Care. 2016;12(2):48-58. doi: http://dx.doi.org/10.13175/swjpcc014-16 PDF
August 2015 Imaging Case of the Month
Michael B. Gotway, MD
Department of Radiology
Mayo Clinic Arizona
Scottsdale, AZ
Clinical History: A 69-year-old man with a history of hairy cell leukemia, in remission, and “smoldering” multiple myeloma (IgG kappa and M-spike with IgM kappa light chain), as well as obstructive sleep apnea treated with continuous positive airway pressure, presents with slowly progressive dyspnea, occasional cough (sometimes productive of yellow sputum) and fatigue, the latter associated with difficulty sleeping and daytime somnolence. Overnight oximetry disclosed 75% of the patient’s oxygen saturations were less than 90%. He is a former smoker (2.5 cigarettes / day for 15 years), but uses cannabis chronically. A chest radiograph (Figure 1) was performed.

Figure 1. Frontal (A) and lateral (B) chest radiography.
Which of the following statements regarding the chest radiograph is most accurate? (Click on the correct answer to proceed to the second of nine panels)
Reference as: Gotway MB. August 2015 imaging case of the month. Southwest J Pulm Crit Care. 2015;11(2):70-81. doi: http://dx.doi.org/10.13175/swjpcc108-15 PDF
Medical Image of the Week: Pott’s Disease

Figure 1. Axial CT scan showing a heterogeneous dense mass-like consolidation in the medial aspect of the right lung apex (arrow).

Figure 2. MRI C-spine (axial T2-weighted images). Panel A: soft tissue marrow edema surrounding the posterior process of the C7 vertebral body and it’s contiguous with a heterogeneous infiltrative process of the right medial lung apex (arrow). Panel B: C7 vertebral body compression (arrow).

Figure 3. Right upper lung biopsy showing necrotizing granulomas (arrow) and histiocytes aggregates.
A 22 year-old man with a history of asthma presented with a two-month history of progressive right upper extremity weakness with back pain, weight loss, and night sweats. CT scan of the chest revealed mass-like infiltrative mass in the right lung apex with mediastinal and hilar lymphadenopathy (Figure 1). An MRI cervical spine showed a large infiltrating process at the right medial lung apex with vertebral body compression (Figure 2).
A CT-guided lung biopsy was performed and it showed necrotizing granulomatous inflammation (Figure 3). Pott’s disease was diagnosed and the patient started on anti-tuberculous treatment with a good recovery.
Pott’s disease is a common cause of spinal infection and its clinical presentations are nonspecific. Early findings on imaging may reveal loss of vertebral body height, bone sequestration, sclerosis, and paraspinal mass with calcification (1). A diagnosis of this condition must be made early as prompt treatment may reduce significant morbidity such as spine deformities to neurologic deficits.
Choua Thao MD1, David G. Kuykendall MD2, Matthew P. Schreiber MD, MHS4, and Carmen Luraschi MD3
University of Nevada School of Medicine: Las Vegas
1Department of Internal Medicine
2Department of Family Medicine
3Division of Pulmonary and Critical Care
Las Vegas, NV
4MedStar Georgetown University Hospital/Washington Hospital Center, Washington, DC
Reference
- Rivas-Garcia A, Sarria-Estrada S, Torrents-Odin C, Casas-Gomila L, Franquet E. Imaging findings of Pott's disease. Eur Spine J. 2013;22:567-78. [CrossRef] [PubMed]
Reference as: Thao C, Kuykendall DG, Schreiber MP, Luraschi C. Medical image of the week: Pott's disease. Southwest J Pulm Crit Care. 2015;11(1):36-7. doi: http://dx.doi.org/10.13175/swjpcc066-15 PDF
Medical Image of the Week: Granulomatous Amoebic Encephalitis

Figure 1. Progressively worsened encephalitis with increasing T2/FLAIR hyperintensity, with restricted diffusion and increasing cortical enhancement in the left anterior/medial temporal lobe and inferior frontal lobe, multifocal areas of hemorrhage, mass effect and interval development of multiple progressive areas of rim enhancement with small areas of restricted diffusion suggested new abscess formation.

Figure 2. Necrotizing granulomas with acute inflammation and microorganisms with the morphologic features of amoeba (H & E stained slides: 500X and 1000X).
A 64-year-old woman with history of deceased donor kidney transplantation presented with altered mental status. MRI of the brain showed new region of T2/FLAIR hyperintensity with restricted diffusion and slight cortical enhancement in the left middle temporal lobe (Figure 1, Panel A). Her neurological exam was notable for expressive aphasia and right-sided weakness. Initial diagnosis of ischemic stroke was further evaluated due to immunosuppressive status. Her CSF showed a WBC of 12 cells/microL with 80% lymphocytes, glucose 61 mg/dL, and protein 53 mg/dL. Follow up MRI showed progression of T2/FLAIR hyperintensity, intraparenchymal hemorrhage, and peripheral patchy enhancement in the left anterior/medial temporal lobe and inferior frontal lobe suspicious for encephalitis (Figure 1, Panel B). Left temporal lobe biopsy revealed granulomatous encephalitis with microorganisms morphologically consistent with amoeba (Figure 2), and tissue cultures grew MRSA. Acanthamoeba species was confirmed by the Centers for Disease Control and Prevention (CDC) with antibody testing. Immunosuppression was tapered. She was treated with vancomycin and a CDC approved regimen of pentamidine, sulfadiazine, flucytosine, fluconazole, azithromycin, and miltefosine. Repeat MRI revealed continued progression of encephalitis with increased T2/FLAIR hyperintensity, mass effect, multifocal hemorrhage and new abscess formation (Figure 1, Panel C). Despite aggressive medical management, her neurologic status continued to deteriorate. Given her grim prognosis and failure to show clinical improvement, her family decided to pursue hospice care.
Granulomatous amebic encephalitis is a life-threatening central nervous system infection caused by the free-living amoebae Acanthamoeba spp., Balamuthia mandrillaris and Sappinia pedata. Onset is subacute to chronic affecting predominantly the immunocompromised population. The diagnosis requires high index of suspicion, and early diagnosis is crucial to survival. Radiological findings are nonspecific and can be seen in CNS tuberculosis, neurocysticercosis, disseminated encephalomyelitis, viral encephalitis etc. Multiple antibiotics targeting various proteins or receptors are required for successful treatment. A combination of surgical and medical interventions may be required to prevent morbidity and mortality.
Ateefa Chaudhury MD1, Christopher Geffre MD2, and Tauseef Afaq Siddiqi MD3
1 Department of Medicine
2 Department of Pathology
3 Division of Pulmonary, Allergy, Critical Care and Sleep Medicine
The University of Arizona, Tucson, AZ
Reference
-
Parija SC, Dinoop K, Venugopal H. Management of granulomatous amebic encephalitis: Laboratory diagnosis and treatment. Trop Parasitol. 2015;5(1):23-8. [CrossRef] [PubMed]
Reference as: Chaudhury A, Geffre C, Siddiqi TA. Medical image of the week: granulomatous amoebic encephalitis. Southwest J Pulm Crit Care. 2015;10(6):330-1. doi: http://dx.doi.org/10.13175/swjpcc051-15 PDF
Medical Image of the Week: Actinomycosis

Figure 1. Thoracic CT scan showing right-sided necrotizing pneumonia, lung abscess and empyema (arrows).

Figure 2. Cytospin and cell block of right lower lobe bronchoalveolar lavage fluid stained with Grocott-Gomori's (or Gömöri) methenamine silver (GMS) stain showing positive filamentous organisms consistent with Actinomyces species within a background of inflammatory cells.

Figure 3. Low (Panel A) and high power view (Panel B) of the lung showing alveolar septa filled with predominantly acute (neutrophilic) infiltrate.
A 55-year-old man with history of tobacco and alcohol abuse, presented with unresolving pneumonia despite treatment with moxifloxacin. It was thought to be possible coccidioidomycosis and an azole was started. However, he returned with increasing dyspnea and hypoxemia. He had leukocytosis with a thoracic CT revealing a loculated empyema, multifocal necrotizing infection and a large intrapulmonary abscess (Figure 1). He was admitted to MICU, intubated and ventilated. He was in septic shock requiring fluid resuscitation, vasopressors, and broad antibiotics. Bronchoscopy revealed erythematous and edematous airways, with drainage of over one liter of purulent fluid. A chest tube was placed to drain pleural fluid with removal of around two liters of blood-tinged, purulent fluid. His condition worsened with development of disseminated intravascular coagulation leading to hemorrhagic shock. He arrested and died. Gram stain on bronchoalveolar lavage fluid showed mixed gram negative and gram variable rods, and cultures grew lactobacillus species. GMS stain revealed filamentous organisms consistent with Actinomyces (Figure 2).
Necrotizing pneumonia is usually secondary to aspiration of oral bacterial flora, and is usually associated with severe sepsis and acute respiratory failure. The obstruction of the bronchus and blood vessels corresponding to a lung segment leads to decreased perfusion that is often shown on contrast enhanced CT scan. Hence, systemic antibiotic treatment alone is usually not effective. The management of necrotizing pneumonia is multidisciplinary; including adequate antibiotic therapy, mechanical ventilation, closed pleural drainage and supportive care. Despite the serious morbidity, massive parenchymal damage and prolonged hospitalizations, long-term outcome following necrotizing pneumonia is good with multidisciplinary care. If initial medical therapy fails, surgery is a reasonable option. Resection of gangrenous lung parenchyma and drainage of pleural empyema can lead to recovery in up to 80% of patients. Rarely, lobectomy can be a salvage operation. Outcome is affected by the severity of disease and underlying comorbidities. It should be considered once operative risk is acceptable.
Tauseef Afaq Siddiqi MD1,2, Tracy Lundberg MD3, Jennifer Thorn MD3, and Dena L’heureux MD1,2
1Division of Pulmonary, Allergy, Critical Care, and Sleep Medicine, The University of Arizona Medical Center, Tucson, AZ
2Department of Medicine, Southern Arizona Veterans Administration Health Sciences Center, Tucson, AZ
3Department of Pathology, The University of Arizona Medical Center, Tucson, AZ
References
- Alifano M, Lorut C, Lefebvre A, Khattar L, Damotte D, Huchon G, Regnard JF, Rabbat A. Necrotizing pneumonia in adults: multidisciplinary management. Intensive Care Med. 2011;37(11):1888-9. [CrossRef] [PubMed]
- Schweigert M, Dubecz A, Beron M, Ofner D, Stein HJ. Surgical Therapy for Necrotizing Pneumonia and Lung Gangrene. Thorac Cardiovasc Surg. 2013;61(7):636-41. [CrossRef] [PubMed]
- Tsai YF, Ku YH. Necrotizing pneumonia: a rare complication of pneumonia requiring special consideration. Curr Opin Pulm Med. 2012;18(3):246-52. [CrossRef] [PubMed]
Reference as: Siddiqi TA, Lundberg T, Thorn J, L’heureux D. Medical image of the week: actinomycosis. Southwest J Pulm Crit Care. 2015;10(5):302-3. doi: http://dx.doi.org/10.13175/swjpcc050-15 PDF
Medical Image of the Week: Leukemic Infiltrates

Figure 1. AP portable chest x-ray demonstrating diffuse bilateral infiltrates.
Figure 2. Histology showing extensive interstitial and perivascular lymphocytic infiltrates.

Figure 3. Immunohistochemical staining for CD8 positive T-cell immunophenotype.
A 50 year-old white man with newly diagnosed, acute T-cell prolymphocytic leukemia presented with progressive exertional dyspnea and non-productive cough. The patient was due to meet with his hematologist that day to discuss initiation of treatment. The patient had not noted fever, chills, night sweats, chest pain, or lower extremity swelling. Blood pressure was 112/60 mm Hg, respiratory rate was 36/minute and labored, pulse was 110/minute and temperature was 37 degrees Celsius. Oxygen saturation measured by pulse oximetry was 62% on room air at rest, and rose to 90% after the application of a 100% non-rebreather mask. Diffuse rales were present on chest auscultation. Marked splenomegaly was present on abdominal examination. Peripheral white blood count was 112.2 K/ul with 99% lymphocytes. Smudge cells were noted. Hemoglobin was 12.9 g/dl and platelet count was 93K/ul. Procalcitonin level was 0.3 pg/ml. The chest radiograph demonstrated diffuse bilateral infiltrates (Figure 1). The patient developed rapidly progressive hypoxemia, was intubated orally, and mechanical ventilation was initiated. Lung biopsies were performed via a video-assisted thoracic surgical approach of the right middle and right lower lobes. Microscopic examination demonstrated extensive leukemic infiltration of the pulmonary interstitium and perivascular space (Figure 2). Immunohistochemical staining showed that the infiltrating cells expressed a CD8 positive T-cell immunophenotype (Figure 3) pattern similar to the patient’s peripheral blood flow cytometry study. Therapy began with an escalating dose of alemtuzumab and intermittent pentostatin, but the patient developed progressive multi-organ failure and expired.
Acute T-cell prolymphocytic leukemia is an aggressive mature T-cell leukemia usually characterized by peripheral blood lymphocytosis and splenomegaly (1). Extramedullary involvement most commonly affects the skin (2). Diffuse interstitial and perivascular pulmonary involvement with respiratory failure has not been previously reported. Pathological involvement of the pulmonary interstitial space should be considered in patients with acute T-cell prolymphocytic leukemia and respiratory insufficiency.
Charles J. VanHook1, Carlyne Cool2, Todd DeBoom3, Robert Fisher4, and
Douglas J. Tangel1
1Department of Intensive Care Medicine
Longmont United Hospital
Longmont, CO
2Department of Pathology and Department of Medicine
University of Colorado and National Jewish Health
Denver, CO
3Department of Pathology
Longmont United Hospital
Longmont, CO
4Department of Oncology
Longmont United Hospital
Longmont, CO
References
-
Valbuena JR, Herling M, Admirand JH, Padula A, Jones D, Medeiros LJ. T-cell prolymphocytic leukemia involving extramedullary sites. Am J Clin Pathol. 2005;123(3):456-64. [CrossRef] [PubMed]
Reference as: VanHook CJ, Cool C, DeBoom T, Fisher R, Tangel DJ. Medical image of the week: leukemic infiltrates. Southwest J Pulm Crit Care. 2015;10(5):235-7. doi: http://dx.doi.org/10.13175/swjpcc043-15 PDF