
Imaging
Those who care for patients with pulmonary, critical care or sleep disorders rely heavily on chest radiology and pathology to determine diagnoses. The Southwest Journal of Pulmonary, Critical Care & Sleep publishes case-based articles with characteristic chest imaging and related pathology.
The editor of this section will oversee and coordinate the publication of a core of the most important chest imaging topics. In doing so, they encourage the submission of unsolicited manuscripts. It cannot be overemphasized that both radiologic and pathologic images must be of excellent quality. As a rule, 600 DPI is sufficient for radiographic and pathologic images. Taking pictures of plain chest radiographs and CT scans with a digital camera is strongly discouraged. The figures should be cited in the text and numbered consecutively. The stain used for pathology specimens and magnification should be mentioned in the figure legend. Those who care for patients with pulmonary, critical care or sleep disorders rely heavily on chest radiology and pathology to determine diagnoses. The Southwest Journal of Pulmonary, Critical Care & Sleep publishes case-based articles with characteristic chest imaging and related pathology. The editor of this section will oversee and coordinate the publication of a core of the most important chest imaging topics. In doing so, they encourage the submission of unsolicited manuscripts. It cannot be overemphasized that both radiologic and pathologic images must be of excellent quality. As a rule, 600 DPI is sufficient for radiographic and pathologic images. Taking pictures of plain chest radiographs and CT scans with a digital camera is strongly discouraged. The figures should be cited in the text and numbered consecutively. The stain used for pathology specimens and magnification should be mentioned in the figure legend.
January 2022 Medical Image of the Month: Bronchial Obstruction Due to Pledget in Airway Following Foregut Cyst Resection

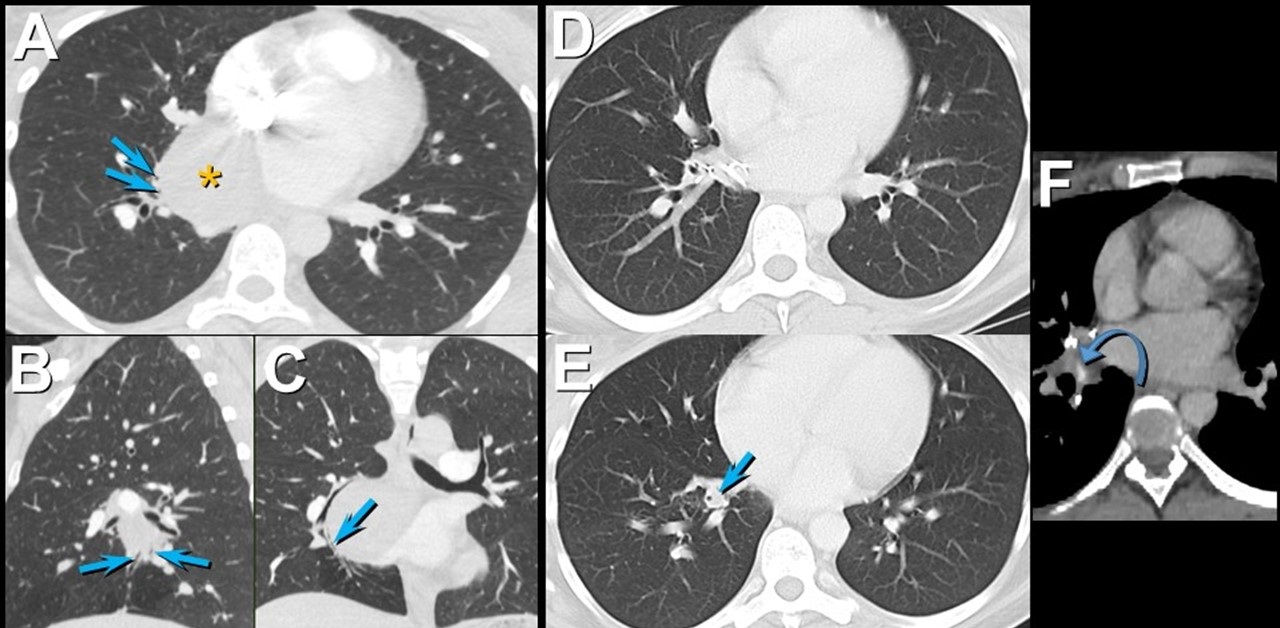
Figure 1. Enhanced chest CT in axial (A), sagittal (B), and coronal (C) planes shows a mediastinal foregut duplication cyst (*) compressing medial basal subsegmental airways (arrows). Axial enhanced chest CT displayed in lung (A and B) and soft tissue (C) windows 7 years after surgical resection of the foregut duplication cyst shows post-resection changes with a focus of hyperattenuation (curved arrow) related to the medial basal segmental bronchus; this bronchus is dilated and fluid-filled more distally (arrow). Click here to view Figure 1 enlarged in a new window.
{kind=link}

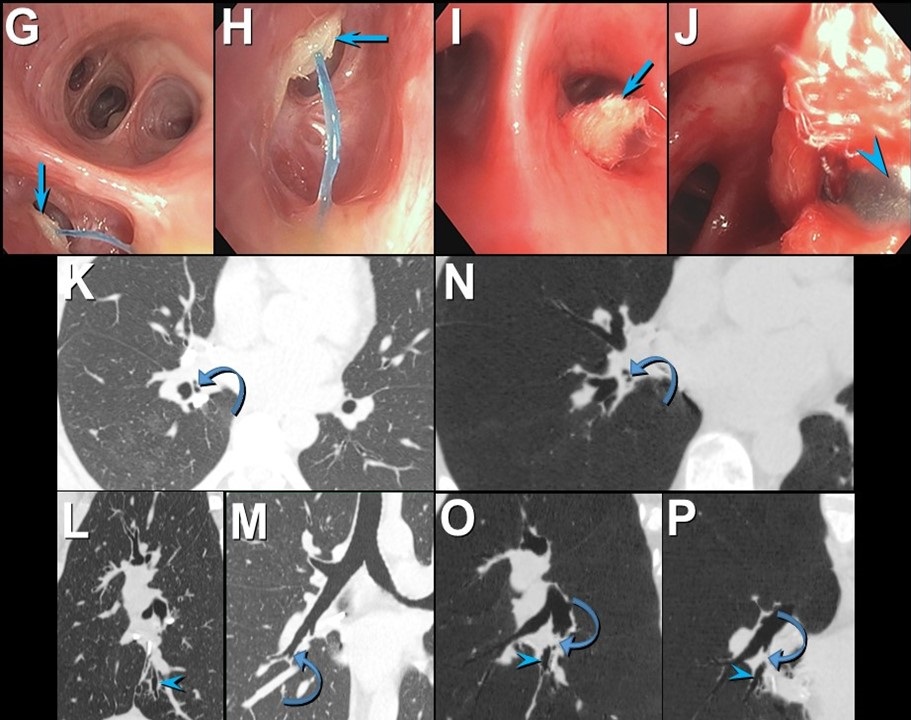
Figure 2. Bronchoscopic images (G-J) show an object obstructing the medial basal segmental right lower lobe bronchus (arrow); a blue suture is attached to the object. The object (arrow) was retrieved using forceps (arrowhead) and was found to reflect a surgical pledget. Follow up unenhanced axial (K), sagittal (L), and coronal (M) chest CT shows mildly stenosed medial basal subsegmental bronchi (curved arrow) with distal bronchiectasis (double arrowheads); these airway abnormalities are shown to advantage using minimum intensity projected images (N-P). Click here to view Figure 2 enlarged in a new window.
{kind=link}
A 37-year-old woman complaining of chest pain and cough underwent resection of a mediastinal foregut duplication cyst complicated by a 10-day hospitalization with a prolonged air leak. Seven years later, she presented with worsening cough and shortness of breath, complaining of similar symptoms intermittently in the 7 years between her surgery and presentation. Chest CT showed a hyperattenuating lesion obstructing the medial basal segmental airways (Figure 1). Bronchoscopy revealed a suture and a pledget obstructing the medial basal segmental right lower lobe bronchus (Figure 2). The pledget and suture were successfully removed. Repeat bronchoscopy several months later showed no residual airway foreign body, although medial basal subsegmental bronchial stenosis prevented advancement of the bronchoscope distally; this finding correlated with the CT impression of airway stenosis or occlusion in this region on the follow up CT.
Bronchogenic cysts result from abnormal lung budding and development of the ventral foregut during the first trimester (1). Many lesions are detected asymptomatically, but larger lesions, as in this patient, may induce symptoms prompting resection. The surgical note for this patient suggested the lesion resided in the right lower lobe, but most bronchogenic cysts arise in the mediastinum near the carina, and this patient’s large lesion extended from the subcarinal space into the azygoesophageal recess. It is possible the surgeon entered the right lower lobe to resect the lesion, resulting in the post-surgical air as well as the surgical pledgets in the medial basal right lower lobe airway that caused the patient’s recurrent chest complaints.
Prasad M. Panse MD1 and Kenneth K. Sakata MD2
Departments of Radiology1 and Pulmonary Medicine2
Mayo Clinic Arizona, Scottsdale, AZ USA
Reference
- Panchanatheeswaran K, Dutta R, Singh KI, Kumar A. Eleven-year experience in thoracoscopic excision of bronchogenic cyst. Asian Cardiovasc Thorac Ann. 2012; 20(5):570-574 perspective. Natl J Maxillofac Surg. 2015; 6(2):144-1451. [CrossRef][PubMed]
Cite as: Panse PM, Sakata KK. January 2022 medical image of the month: bronchial obstruction due to pledget in airway following foregut cyst resection. Southwest J Pulm Crit Care. 2022;24(1):6-7. doi: https://doi.org/10.13175/swjpcc065-21 PDF
May 2017 Imaging Case of the Month
Prasad M. Panse, MD and Michael B. Gotway, MD
Department of Radiology
Mayo Clinic Arizona
Scottsdale, Arizona USA
Clinical History: Clinical History: A 32-year-old man presented for routine physical examination. His past medical history is unremarkable and the physical examination and basic laboratory data were within normal limits.
A frontal chest radiograph (Figure 1) was performed.

Figure 1: Frontal (A) and lateral (B) chest radiography.
Which of the following statements regarding the chest radiograph is most accurate? (Click on the correct answer to proceed to the second of nine pages)
- The frontal chest radiograph shows an abnormal mediastinal contour
- The frontal chest radiograph shows basal predominant fibrotic abnormalities
- The frontal chest radiograph shows large lung volumes with a cystic appearance
- The frontal chest radiograph shows multifocal small pulmonary nodules
- The frontal chest radiograph shows no abnormal findings
Cite as: Panse PM, Gotway MB. May 2017 imaging case of the month. Southwest J Pulm Crit Care. 2017;14(5):201-12. doi: https://doi.org/10.13175/swjpcc055-17 PDF
Medical Image of the Week: Arachnoid Cyst

Figure 1. Axial T1 MRI of mass.

Figure 2. Coronal T2 weighted MRI demonstrating compressions onto mesial temporal lobes and stretching of the optic chiasm and tracts; upward displacement of the hypothalamus, third ventricle small in caliber and mild posterior displacement of the midbrain.
A 40 year-old woman with adult attention deficit hyperactive and bipolar 1 disorder presents with an altered mental status. Per her family, she had been non-verbal, with reduced oral intake, confusion and sedated for the past three days. Per her husband, she had episodes of diarrhea and abdominal discomfort. She was on multiple medications including ramelteon 8mg nightly, atomoxetine 40mg daily, hydroxyzine 25mg twice daily, bupropion 75mg twice daily and risperidone 2mg daily with recent addition of lithium ER 1200mg/daily started one month prior to presentation with unknown adherence.
Upon arrival, vital signs were within normal limits. Physical exam revealed an overweight Caucasian woman with a significant coarse tremor visible at rest, restlessness and diaphoresis. Neurological examination was limited by patient hesitancy, however, it did not demonstrate focal deficits except for altered consciousness with Glasgow Coma Scale of 10. Notable laboratory findings were Na+ 134 mEq/L, K+ 3.2 mEq/L, and lithium level of 3.9 mmol/L, urine toxicology positive for cocaine, and EKG showed QT prolongation. Toxicology and psychiatry were consulted.
CT of her head without contrast showed a large midline lesion in the sellar/suprasellar estimated to be 5.2x 2.1x 3.2cm. On hospital day number 2 the patient was more somnolent with down trending lithium level of 2.6 mmol/L. Later that day the patient had an observed generalized tonic clonic seizure which required abortive therapy with lorazepam and levetiracetam. A MRI revealed large arachnoid cyst measuring 3.6x3.1x3.5cm causing mass effect on adjacent tissue. (Figures 1 and 2). Neurology was consulted and recommended neurosurgery evaluation who deferred intervention to an outpatient basis given her lithium overdose as a more likely etiology of her seizure and not the arachnoid cyst.
Arachnoid cysts are cerebral spinal fluid filled sacs located between the brain or spinal cord and the arachnoid membrane. They can be either primary, which are present at birth due to developmental abnormalities of the brain and spinal cord, or they may be secondary, which are the result of head injury, meningitis, tumors, or a complication of brain surgery. Symptoms are based on the size and location of the cyst and include headache, nausea and vomiting, seizures, hearing and visual disturbances, vertigo, and difficulties with balance and walking. If the cyst compresses the spinal cord or nerve roots, then individual may experience progressive back and leg pain and tingling or numbness in the legs or arms.
Diagnosis is usually via MRI which distinguishes between fluid-filled arachnoid cysts from other types of cysts. The treatment depends on the location and the size of the cyst. If the cyst is small and does not compress any of the surrounding structures, with an absence of symptoms, no treatment is necessary. The two main ways of treating symptomatic cysts include surgery or placing a permanent shunt to drain the fluid. Surgical approaches include microscopic open surgical fenestration procedure in which the neurosurgeon opens the skull to gain access to the cyst, then opens the cyst to release pressure, allowing contents to be absorbed by the brain. Another surgical approach involves endoscopic cyst fenestration in which an endoscope is used to drain the cyst internally without having to perform an open surgery. In some instances, formal craniotomy with excision/marsupialization of the cyst into the subarachnoid space is performed. The procedure performed depends on the surgeon’s comfort with the technique and the size/location of the cyst.
Matthew Erisman MD, Rozina Parbtani MS IV, and Faraz Jaffer MD.
Department of Internal Medicine
University of Arizona at South Campus
Tucson, Arizona USA
References
- Al-Holou WN, Terman S, Kilburg C, Garton HJ, Muraszko KM, Maher CO. Prevalence and natural history of arachnoid cysts in adults. J Neurosurg. 2013 Feb;118(2):222-31. [CrossRef] [PubMed]
- Eidlitz-Markus T, Zeharia A, Cohen YH, Konen O. Characteristics and management of arachnoid cyst in the pediatric headache clinic setting. Headache. 2014 Nov-Dec;54(10):1583-90. [CrossRef] [PubMed]
Cite as: Erisman M, Parbtani R, Jaffer F. Medical image of the week: arachnoid cyst. Southwest J Pulm Crit Care. 2016;13(4):181-3. doi: http://dx.doi.org/10.13175/swjpcc074-16 PDF
June 2015 Imaging Case of the Month
Michael B. Gotway, MD
Department of Radiology
Mayo Clinic Arizona
Scottsdale, AZ
Clinical History: A 58-year-old man presented for a pre-operative evaluation for surgery planned for resection of localized prostate malignancy. A frontal chest radiograph (Figure 1) was performed.

Figure 1. Figure 1: Frontal (A) and lateral (B) chest radiography.
Which of the following statements regarding the chest radiograph is most accurate? (Click on the correct answer to proceed to the second of seven panels)
Reference as: Gotway MB. June 2015 imaging case of the month. Southwest J Pulm Crit Care. 2015;10(6):332-40. doi: http://dx.doi.org/10.13175/swjpcc078-15 PDF