
Imaging
Those who care for patients with pulmonary, critical care or sleep disorders rely heavily on chest radiology and pathology to determine diagnoses. The Southwest Journal of Pulmonary, Critical Care & Sleep publishes case-based articles with characteristic chest imaging and related pathology.
The editor of this section will oversee and coordinate the publication of a core of the most important chest imaging topics. In doing so, they encourage the submission of unsolicited manuscripts. It cannot be overemphasized that both radiologic and pathologic images must be of excellent quality. As a rule, 600 DPI is sufficient for radiographic and pathologic images. Taking pictures of plain chest radiographs and CT scans with a digital camera is strongly discouraged. The figures should be cited in the text and numbered consecutively. The stain used for pathology specimens and magnification should be mentioned in the figure legend. Those who care for patients with pulmonary, critical care or sleep disorders rely heavily on chest radiology and pathology to determine diagnoses. The Southwest Journal of Pulmonary, Critical Care & Sleep publishes case-based articles with characteristic chest imaging and related pathology. The editor of this section will oversee and coordinate the publication of a core of the most important chest imaging topics. In doing so, they encourage the submission of unsolicited manuscripts. It cannot be overemphasized that both radiologic and pathologic images must be of excellent quality. As a rule, 600 DPI is sufficient for radiographic and pathologic images. Taking pictures of plain chest radiographs and CT scans with a digital camera is strongly discouraged. The figures should be cited in the text and numbered consecutively. The stain used for pathology specimens and magnification should be mentioned in the figure legend.
October 2023 Medical Image of the Month: Swyer-James-MacLeod Syndrome
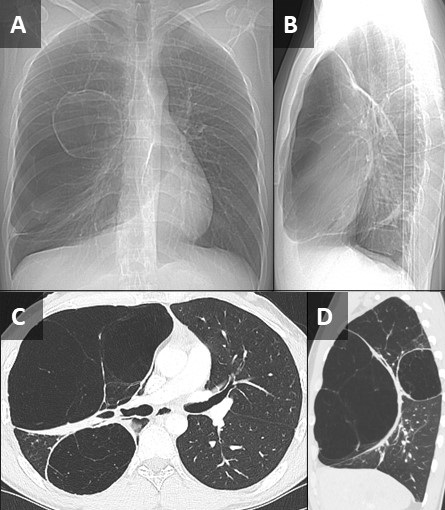
 Figure 1. Frontal (A) and lateral (B) topographic images from a non-contrast chest CT show a relative paucity of lung markings in the right hemithorax. There are at least 2 large, cystic-appearing lesions in the right lung, which appears somewhat hyperinflated. Axial (C) and sagittal (D) reconstructions from the CT confirm unilateral areas of emphysematous appearing hyperinflated lung with surrounding atelectasis. The left lung appears relatively normal. Click here to view Figure 1 in an enlarged, separate window.
Figure 1. Frontal (A) and lateral (B) topographic images from a non-contrast chest CT show a relative paucity of lung markings in the right hemithorax. There are at least 2 large, cystic-appearing lesions in the right lung, which appears somewhat hyperinflated. Axial (C) and sagittal (D) reconstructions from the CT confirm unilateral areas of emphysematous appearing hyperinflated lung with surrounding atelectasis. The left lung appears relatively normal. Click here to view Figure 1 in an enlarged, separate window.
{kind=link}
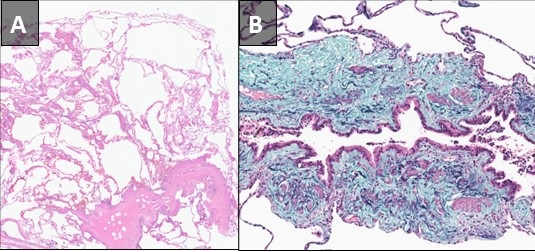
 Figure 2. Hematoxylin and Eosin stained low-power pathological image from right upper lobectomy (A) demonstrates chronic bronchiolitis with features of subtotal obliterative bronchiolitis associated with mild septal fibrosis and prominent emphysematous/cystic change. Elastic trichrome stain of a small airway (B) demonstrates subtotal bronchiolitis obliterans. Click here to view Figure 2 in an enlarged, separate window.
Figure 2. Hematoxylin and Eosin stained low-power pathological image from right upper lobectomy (A) demonstrates chronic bronchiolitis with features of subtotal obliterative bronchiolitis associated with mild septal fibrosis and prominent emphysematous/cystic change. Elastic trichrome stain of a small airway (B) demonstrates subtotal bronchiolitis obliterans. Click here to view Figure 2 in an enlarged, separate window.
{kind=link}
Pathological slides from a right upper lobectomy specimen obtained at an outside institution were submitted to our Department of Pathology for review. A pre-operative noncontrast chest CT from the outside institution was submitted along with the path slides. The patient was a 27 y/o man who presented to the outside institution with exercise intolerance and increasing shortness of breath following a bout of COVID in early 2023. The patient also related a history of possible chronic myocarditis. A review of the CT demonstrated 2 distinct right-sided areas of hyperinflated, emphysematous lung with a relatively normal appearing left lung (Figure 1). Although congenital lobar emphysema was considered, the multifocal nature of the findings suggested against this, and a diagnosis of Swyer-James-MacLeod Syndrome was entertained. Histopathological analysis (Figure 2) confirmed this suspicion. When questioned further, the patient related a history of neonatal RSV infection requiring 3 weeks of hospitalization. The constellation of historical, radiological, and pathological findings was consistent with Swyer-James- MacLeod Syndrome.
This syndrome was first described in 1949 in a case report of a six-year-old boy from the UK by pediatrician Paul Swyer and radiologist George James (1). The pulmonologist William MacLeod published a review of nine cases in 1954 (2). Also known as “unilateral hyperlucent lung syndrome”, this is a postinfectious form of bronchiolitis obliterans. Severe infection early in life, while the lungs are still developing, is the proposed mechanism. Although different infections organisms are associated with this, respiratory syncytial virus is most implicated. Swyer-James-MacLeod Syndrome usually affects the lungs asymmetrically. On imaging, the most common pattern is that of a unilateral hyperlucent lung which may or may not be associated with hyperinflation and may or may not be associated with bronchiectasis (3). There is reduction in pulmonary blood flow and formation of septal fibrosis which leads to obstruction of pulmonary capillary beds. Alveolar hyperinflation leads to mechanical resistance to pulmonary blood flow and reduced ventilation leads to pulmonary vasoconstriction. Most patients asymptomatic, and many cases discovered incidentally. Treatment is usually conservative and preventative, focused on controlling pulmonary infections. Inhaled corticosteroids may have a limited role in treatment as well (4).
Samantha Moore, MD, PhD1 and Clinton Jokerst MD2
Department of Laboratory Medicine and Pathology1 and Department of Radiology2
Mayo Clinic Arizona, Scottsdale, AZ USA
References
- Swyer PR, James GC. A case of unilateral pulmonary emphysema. Thorax. 1953 Jun;8(2):133-6. [CrossRef] [PubMed]
- William Mathieson Macleod. Lancet. 1977 Oct 15;2(8042):833. [PubMed]
- Lucaya J, Gartner S, García-Peña P, Cobos N, Roca I, Liñan S. Spectrum of manifestations of Swyer-James-MacLeod syndrome. J Comput Assist Tomogr. 1998 Jul-Aug;22(4):592-7. [CrossRef] [PubMed]
- Mehra S, Basnayake T, Falhammar H, Heraganahally S, Tripathi S. Swyer-James-MacLeod syndrome-a rare diagnosis presented through two adult patients. Respirol Case Rep. 2017 Jun 16;5(5):e00245. [CrossRef] [PubMed]
Medical Image of the Month: Mounier-Kuhn Syndrome

Figure 1. AP chest x-ray showing significant tracheomegaly (diameter 30.8 mm), bilateral interstitial infiltrates with dense consolidation more at the lower lobes (left>right).

Figure 2. Axial thoracic CT in lung windows (A-D) and soft tissue windows (E-F). Sagittal CT in soft tissue windows (G-H). A: tracheal diameters in 2 dimensions (coronal 30.4 mm, sagittal 37.6 mm), para-septal emphysema (yellow arrows). B: showing tracheomegaly (23.2 x 34.3 mm) and para-septal emphysema changes (yellow arrows. C: enlarged mainstem bronchi diameters (right mainstem 22.3 x 30.6 mm, left mainstem 24.4 x 16.0 mm). In addition to central bronchiectatic changes (red arrows), left lower lobe consolidative changes (blue arrow). D: dense left lower lobe consolidation and para-septal emphysema. E: Significant tracheomegaly (31.5 x 41.a mm) and dilated esophagus (orange arrow). F: Significant tracheomegaly and dilated esophagus.

Figure 3. A: Sagittal CT scan (soft tissue window) showing significant tracheomegaly (sagittal diameter 35.8 mm). B: Sagittal CT chest (lung window) showing significant tracheomegaly, multiple tracheal diverticuli (green arrows) on the upper posterior tracheal wall.

Figure 4. Pulmonary function testing.
A 52-year-old non-smoking, Caucasian male patient with a past medical history of reported chronic obstructive pulmonary disease (COPD), recurrent lower respiratory tract infections, prior history of pneumothorax, and dysphagia presented with fevers and shortness of breathing associated with a productive cough for one week. Clinically, he was mildly tachypneic and chest auscultation revealed crackles bilaterally - more prominent at the left base. A chest radiograph (Figure 1) showed bilateral lower lobe pulmonary opacities (left more than right). Computed tomography (CT) of the chest demonstrated airspace disease in the lower lobes in addition to significant tracheobronchomegaly along with paraseptal emphysema and central bronchiectatic changes (Figures 2 and 3). Upper posterior tracheal wall diverticulae were also noted (Figure 3). Serum α1-antitrypsin level and serum immunoglobulins, including IgE levels, were normal. Our patient declined performing diagnostic bronchoscopy. He had a pulmonary function test performed few months prior to his hospital admission which showed combined mild obstructive/restrictive pattern (Figure 4). He responded well to empiric antibiotics and chest percussion therapy. He was discharged in stable condition.
Discussion
On the basis of above findings, a diagnosis of Mounier-Kuhn syndrome complicated by pneumonia was made. The syndrome was first described by P. Mounier-Kuhn in 1932 (1). The diagnosis is usually made when the tracheal diameter is greater than 3 cm on a CT chest (measured 2 cm above the aortic arch) (2). Other diagnostic criteria include a mainstem bronchial diameter of 20-24 mm (right) and 15-23 mm (left) (3). Our patient’s tracheal diameter was around 37 mm. Both mainstem bronchi were dilated.
The abnormal tracheobronchial dilatation in this syndrome is attributed to atrophy of the muscular and elastic tissues in the tracheal and the bronchial walls (3). Hence, in addition to tracheobronchomegaly, these patients can also develop tracheal diverticulosis along with varicose and cystic bronchiectasis (3). These patients usually present in the 3rd or 4th decade of life with nonspecific respiratory symptoms including recurrent bronchitis and subsequently end up being misdiagnosed with COPD (3).
Three subtypes of this syndrome had been described. Subtype 1 has symmetric dilation of the trachea and mainstem bronchi. Subtype 2 demonstrates tracheal dilation and tracheal diverticula. Subtype 3 has diverticular and saccular structures extending to the level of the distal bronchi (3). Our patient likely fits subtype 3 of this syndrome. Overall, treatment is supportive - usually with antibiotics, physiotherapy and postural drainage. In rare instances, tracheal stenting has been used (4). Special consideration should be taken post intubation as achieving good cuff seal can be potentially challenging.
Dysphagia has not been well documented in this syndrome and could be a coincidental finding in our case. However, theoretically, the etiology of this patient’s dysphagia could be secondary to extrinsic compression of the anterior esophageal wall by his markedly dilated trachea. Historically, he underwent multiple esophageal dilatations and at least one Botox injection over the last 5 years without any significant improvement.
Abdulmonam Ali MD and Naga S. Sirikonda MD
Pulmonary and Critical Care
Good Samaritan Hospital
Mount Vernon, Illinois
References
- Mounier-Kuhn P. "Dilatation de la trachee: constatations, radiographiques et bronchoscopies." Lyon Med. 1932;150:106-9.
- Menon B, Aggarwal B, Iqbal A. Mounier-Kuhn syndrome: report of 8 cases of tracheobronchomegaly with associated complications. South Med J. 2008;101(1):83-7. [CrossRef] [PubMed]
- Falconer M, Collins DR, Feeney J, Torreggiani WC. Mounier-Kuhn syndrome in an older patient. Age Ageing. 2008;37(1):115-6. [CrossRef] [PubMed]
- Schwartz M, Rossoff L. Tracheobronchomegaly. Chest 1994;106(5):1589-90. [CrossRef] [PubMed]
Cite as: Ali A, Sirikonda NS. Medical image of the month: Mounier-Kuhn syndrome. Southwest J Pulm Crit Care. 2019;19(2):73-5. doi: https://doi.org/10.13175/swjpcc044-19 PDF
Medical Image of the Week: Yellow Nail Syndrome

Figure 1. Photographs showing the patient’s discolored, yellowish nails.

Figure 2. Representative images from the thoracic CT scan in lung windows showing bronchiectasis most marked in the left upper lobe.
A 67-year-old woman with a previous history of yellow nail syndrome presented with a long history of cough, increased sputum production, recurrent swelling in her lower extremities and recurrent respiratory infections. Physical examination revealed non-pitting edema in the lower extremities and discolored nails (Figure 1). A thoracic CT scan showed bronchiectasis in the left upper lobe (Figure 2). She did not have a history of pleural effusions or chronic sinusitis.
Yellow nail syndrome is very rare disorder associating yellow nail discoloration, bronchiectasis and lymphedema (1). Other frequent manifestations include sinusitis and recurrent pleural effusions. The disease is most frequently isolated but may be associated with other diseases implicating the lymphatic system, autoimmune diseases or cancers. The symptoms result from lymphatic impairment but the cause of the impairment is unknown. Treatment is symptomatic for each component. Vitamin E, combined with fluconazole, is usually prescribed to treat yellow nails and achieves a partial or complete response. Spontaneous resolution is also possible. Although prognosis is usually considered to be good, a Kaplan–Meier survival curve estimated median survival at 132 months, shorter than that of a paired-control population (2).
Lewis J. Wesselius MD
Departments of Pulmonary Medicine
Mayo Clinic Arizona
Scottsdale, AZ USA
References
- Vignes S, Baran R. Yellow nail syndrome: a review. Orphanet J Rare Dis. 2017 Feb 27;12(1):42. [CrossRef] [PubMed]
- Maldonado F, Tazelaar HD, Wang CW, Ryu JH. Yellow nail syndrome: analysis of 41 consecutive patients. Chest. 2008;134:375–81. [CrossRef] [PubMed]
Cite as: Wesselius LJ. Medical image of the week: yellow nail syndrome. Southwest J Pulm Crit Care. 2017;15(4):230-1. doi: https://doi.org/10.13175/swjpcc142-17 PDF
October 2017 Imaging Case of the Month
Paul J. Conomos, MD1
Michael B. Gotway, MD2
1Arizona Pulmonary Specialists
Phoenix, AZ USA
2Mayo Clinic Arizona
Scottsdale, AZ USA
Clinical History: An 18-year-old man with no known previous medical history presented with complaints of intermittent cough persisting several months. No hemoptysis was noted.
Physical examination was largely unremarkable and the patient’s oxygen saturation was 99% on room air. The patient’s vital signs were within normal limits.
Laboratory evaluation was unremarkable. Quantiferon testing for Mycobacterium tuberculosis was negative, and testing for coccidioidomycosis was unrevealing. Frontal and lateral chest radiography (Figure 1) was performed.

Figure 1. Figure 1. Frontal (A) and lateral (B) chest radiography.
Which of the following statements regarding the chest radiograph is most accurate? (Click on the correct answer to proceed to the second of eight pages)
- The chest radiograph shows asymmetric reticulation and interlobular septal thickening
- The chest radiograph shows bilateral reticulation associated with decreased lung volumes
- The chest radiograph shows focal consolidation
- The chest radiograph shows large lung volumes
- The chest radiograph shows small cavitary pulmonary nodules
Cite as: Conomos PJ, Gotway MB. October 2017 imaging case of the month. Southwest J Pulm Crit Care. 2017;15(4):138-46. doi: https://doi.org/10.13175/swjpcc119-17 PDF
Medical Image of the Week: Typical Pulmonary CT Findings Following Radiotherapy

Figure 1. Panel A: CT chest, lung windows, demonstrating a spiculated nodule, biopsy proven adenocarcinoma in the right lower lobe (arrow). Panel B: Eight months post stereotactic radiation therapy, there has been development of focal consolidation, with air bronchograms, involving the right middle and lower lobes. Notice the volumetric appearance. The primary malignancy is no longer identified as such. Panel C: Thirteen months later the consolidation has evolved into an area of volume loss, containing bronchiectasis, and sharp contours as a result of organized fibrosis.
Radiation-induced lung disease (RILD) commonly develops in patients treated with radiation for intrathoracic and chest wall malignancies.
There are two distinct radiographic patterns:
- Radiation pneumonitis which occurs within 4-12 weeks after completion of therapy, and is characterized by development ground-glass opacities and/or consolidation in and around the treated lesion. A somewhat nodular or patchy appearance may occur. Typically, the affected tissue conforms to the radiation ports and may cross fissures/lobes. There may be milder similar changes in the contralateral lung.
- A chronic phase, known as radiation fibrosis, is noticeable about 6-12 months post treatment and may progress up to 2 years, after which the findings tend to stabilize. In this stage, the areas of consolidation undergo volume loss, architectural distortion and may contain traction bronchiectasis. Linear and band scarring may also be seen. In this phase, sharper demarcation between normal and irradiated lung parenchyma is commonly seen.
Special attention to the typical radiological characteristics and timeline, in most cases allows to distinguish RILD from potential superimposed infection, subacute inflammatory diseases, locally recurrent neoplasm and radiation-induced neoplasms.
Andrew Erickson MS IV1, Berndt Schmidt MD2, Veronica Arteaga MD2, Diana Palacio MD2
1Midwestern University – Arizona College of Osteopathic Medicine
2Division of Thoracic Radiology, Department of Medical Imaging. University of Arizona, Tucson (AZ)
Reference
- Choi YW, Munden RF, Erasmus JJ, Joo Park K, Chung WK, Jeon SC, Park CK. Effects of radiation therapy on the lung: radiologic appearances and differential diagnosis. Radiographics. 2004 Jul;24(4):985-97. [CrossRef] [PubMed]
Cite as: Erickson A, Schmidt B, Arteaga V, Palacio D. Medical image of the week: typical pulmonary CT findings following radiotherapy. Southwest J Pulm Crit Care. 2017;15(3):120-1. doi: https://doi.org/10.13175/swjpcc112-17 PDF
Medical Image of the Week: Bronchiectasis

Figure 1. Video of thoracic axial computed tomography (CT) images in lung windows demonstrating dependent cystic bronchiectasis with air-fluid levels.

Figure 2. Video of thoracic coronal CT images.
A 49-year old Native American woman with chronic hypoxic and hypercarbic respiratory failure requiring 3 liters continuous via nasal cannula and nocturnal non-invasive bi-level ventilation presented with acute shortness of breath for 5 days. She has history of recurrent respiratory infections since early childhood, however over the past five years has been treated multiple times for presumed COPD exacerbation with last such treatment one month prior to admission.
Upon arrival, vitals displayed elevated blood pressure 183/96. Clinical examination demonstrated morbidly obese patient in mild somnolence and has diffuse expiratory wheezing, basal crackles with reduced air entry bilaterally. Laboratory examination showed leukocytosis (13,800 cells/uL) with neutrophilic predominance, thrombocytopenia (85,000 cells/uL), and elevated bicarbonate (31 mg/dL). Arterial blood gas showed pH=7.29, pCO2 756 mm Hg, and pO2 73 mm Hg. Thoracic computed tomography (CT) with contrast ruled out pulmonary embolism, however demonstrated extensive cystic bronchiectasis in left upper and lower lobes, right lower lobe along with findings consistent with chronic bronchitis and bronchiolitis. (Figures 1 and 2)
Bronchiectasis workup showed-low serum globulins (IgG 388 mg/dL, IgM 18 mg/dL , IgA 64 mg/dL, with low IgG-1 226 mg/dL, IgG-2 140 mg/dL). Alpha Antitrypsin level was high. Blood culture, sputum culture, urine Legionella, Streptococcus pneumoniae antigen, Coccidioidomycosis serology, quantiferon and AFB stain for TB were all negative. Aggressive nebulization therapy, intermittent Bi-level positive airway pressure and antibiotics allowed her to become stabilized to a baseline oxygen requirement. She was discharged with diagnosis of acute on chronic hypoxic and hypercarbic respiratory failure secondary to flare up of severe bronchiectasis secondary to common variable immunodeficiency (CVID).
Common Variable Immunodeficiency (CVID), a subset of primary humoral immunodeficiency diseases, is a condition of inadequate immunoglobulin expression in response to antigen exposure. Prevalent equally amongst the sexes and ranges from 1 in 10,000 to 50,000 with bimodal incidence either within the first or third decade of life. Initial history is nonspecific, consisting of recurrent episodes of sinusitis and bronchitis with severity of illness dependent on level of immunoglobulin expression. The European Society for Immunodeficiency defines CVID as reduced (below 2 standard deviations of the mean) levels of IgG with reduced IgA and/or IgM, together with failure to mount a significant antibody response to vaccination, in the absence of a known cause. However, etiology of CVID is still incompletely understood and given the clinical heterogeneity in patient presentation, there is lack of consensus on clinical definition. Persistent sinus or respiratory complaints, in combination with finding of airway bronchiectasis lead a referral to an immunologist or pulmonologist in pursuit of diagnosis.
Bronchiectasis, a syndrome characterized by irreversible destruction, abnormal dilatation impairing clearance and leading to mucous pooling, is a common development in this impaired immune condition. Management of disease is multifactorial with symptom control, administration of appropriate immunizations and immunoglobulin replacement in agammaglobulinemia in order to curb recurrence of infections. Pulmonary morbidity due to bronchiectasis is common, however role of lung transplant in this patient population is unknown.
Practitioners should remain cognizant of considering CVID in patients with history of recurrent pneumonias and imaging findings of bronchiectasis to hasten specialty referral early and minimize pulmonary morbidity.
Faraz Jaffer, MD. Nirmal Singh, MD. and Jennifer Huang-Tsang, MD.
Department of Internal Medicine
University of Arizona at South Campus
Tucson, Arizona USA
References
- Panigrahi MK. Common variable immunodeficiency disorder - An uncommon cause for bronchiectasis. Lung India. 2014 Oct;31(4):394-6. [CrossRef] [PubMed]
- Tarzi MD, Grigoriadou S, Carr SB, Kuitert LM, Longhurst HJ.Clinical immunology review series: An approach to the management of pulmonary disease in primary antibody deficiency. Clin Exp Immunol. 2009 Feb;155(2):147-55. [CrossRef] [PubMed]
- Cunningham-Rundles C. How I treat common variable immune deficiency. Blood. 2010 Jul 8;116(1):7-15. [CrossRef] [PubMed]
Cite as: Jaffer F, Singh N, Huang-Tsang J. Medical image of the week: bronchiectasis. Southwest J Pulm Crit Care. 2016;12(6):258-60. doi: http://dx.doi.org/10.13175/swjpcc045-16 PDF
Medical Image of the Week: Right Middle Lobe Syndrome

Figure 1. Panel A: PA chest x-ray showing calcified mediastinal lymphadenopathy. Panel B: Lateral view showing a triangle of increased density between the minor fissure and the lower half of the major fissure seen on the lateral view (blue arrow) .

Figure 2. Image from the thoracic CT scan in lung windows showing calcified mediastinal lymph notes (green arrows).
A 73 year-old woman, a lifetime non-smoker, presented to the pulmonary clinic with chronic dyspnea on exertion and cough. Physical exam was unremarkable and pulmonary function testing showed normal spirometry. A chest radiograph revealed calcified mediastinal adenopathy and increased density in the right middle lobe region (Figure 1). A computed tomography scan of the chest revealed significant narrowing of the right middle lobe bronchus with partial atelectasis and prominent calcified mediastinal lymphadenopathy (Figure 2). Bronchoscopy showed no endobronchial lesions but there was evidence of extrinsic compression surrounding the right middle lobe orifice. An endobronchial biopsy revealed noncaseating granulomas. Bronchoscopy cultures and cytology were negative and this was presumed to be from a previous infection with histoplasmosis given the patient’s long-term residence in an endemic area. Given chronic narrowing of right middle lobe bronchus with persistent atelectasis of the right middle lobe, the patient was diagnosed with right middle lobe syndrome. She was started on combination therapy with a long-acting beta agonist and inhaled corticosteroid with complete resolution of her symptoms.
Right middle lobe syndrome (RMLS) is defined as recurrent or chronic atelectasis of the right middle lobe. Although more commonly described in children, it is becoming more prevalent in adults with a predilection for women. There are two distinct types of pathophysiology- obstructive and non-obstructive. Obstructive pathophysiology is defined when there is an endobronchial lesion or extrinsic compression of the middle lobe bronchus by lymphadenopathy (as in our case) or a tumor. Non-obstructive pathophysiology occurs when there is recurrent infection or inflammation leading to bronchiectasis and scarring. Certain anatomical characteristics, including the acute take-off angle of the right middle lobe bronchus create poor conditions for drainage and collateral ventilation (1).
Symptoms of RMLS include chronic or recurrent cough, dyspnea, wheezing and recurrent infections. High resolution computed tomography of the chest is the gold standard for imaging, as this will show narrowing of the right middle lobe orifice along with etiologies of extrinsic compression (Figure 2). Patients suspected of having RMLS warrant a bronchoscopy to evaluate for patency of right middle lobe bronchus, to exclude malignancy and for evaluation of infectious etiologies (1). The treatment of RMLS includes bronchodilator therapy along with mucolytics, chest physiotherapy and antibiotics if bronchiectasis is problematic. Lobectomy may be warranted if malignancy is diagnosed, aggressive medical management fails or hemoptysis occurs (2).
Elaine A. Cristan, MD and Linda Snyder, MD
Department of Medicine
Division of Pulmonary, Critical Care, Sleep and Allergy Medicine
Banner University Medical Center
Tucson, AZ USA
References
-
Gudbjartsson T, Gudmundsson G. Middle lobe syndrome: a review of clinicopathological features, diagnosis and treatment. Respiration. 2012;84(1):80-6. [CrossRef] [PubMed]
-
Einarsson JT, Einarsson JG, Isaksson H, Gudbjartsson T, Gudmundsson G. Middle lobe syndrome: a nationwide study on clinicopathological features and surgical treatment. Clin Respir J. 2009 Apr;3(2):77-81. [CrossRef] [PubMed]
Cite as: Cristan EA, Snyder L. Medical image of the week: right middle lobe syndrome. Southwest J Pulm Crit Care. 2016; May;12(5):199-200. doi: http://dx.doi.org/10.13175/swjpcc030-16 PDF
Medical Image of the Week: Kartagener Syndrome

Figure 1. Panel A: AP chest x-ray showing dextrocardia with left sided pneumothorax. Panel B: CT Chest lung windows showing diffuse bronchiectasis. Panel C: CT Abdomen consistent with situs inversus.
A 65-year-old woman presented with 7 days of productive cough and the new onset sharp central chest pain. She has a known history of chronic sinusitis and COPD after being a 50 pack-year smoker. On examination, her blood pressure was 116/70 with a heart rate of 86 (sinus rhythm) and oxygen saturations were 93% on 4L/min by nasal cannula. She had bilateral expiratory wheezes with reduced air entry on the left side.
An AP chest x-ray revealed dextrocardia with a left sided tension pneumothorax (Figure 1A). Our patient was stabilized with an urgent chest tube insertion and taken for a CT chest and abdomen. CT chest indicated diffuse bronchiectasis (Figure 1B, arrow) with a CT of the abdomen showing reversal of major abdominal organs (Figure 1C).
First described in 1933, the triad of chronic sinusitis, bronchiectasis, and situs inversus is classic for Kartagener syndrome (1). Otherwise known as primary ciliary dyskinesia, it is an autosomal recessive disorder affecting the dynein motor protein on microtubules. Ciliary dysfunction from an embryonic stage is the underlying cause for 50% of patients with situs inversus (2). Ongoing difficulties clearing mucous and secretions from abnormal ciliary movements accelerates the development of rhinosinusitis and bronchiectasis (3). Fertility is also a common concern with most males being infertile and females having a lower likelihood of successful pregnancy (4).
Confirmatory testing requires electron microscopy to determine ultrastructure and high-speed video microscopy to determine abnormal movement of cilia (4). Long-term management involves control of respiratory complications with regular spirometry and pulmonary follow up.
Debraj Das, MD
Department of Medicine
Faculty of Medicine and Dentistry
University of Alberta
Edmonton, AB, Canada
References
-
Kartagener M. Zur pathogenese der bronchiectasien. I Mitteilung: bronchiectasien bei situs viscerum inversus. Betr Klin Tuberk. 1933; 83:498-501.
-
Noone PG, Leigh MW, Sannuti A, et al. Primary ciliary dyskinesia: diagnostic and phenotypic features. Am J Respir Crit Care Med. 2004; 169:459-467. [CrossRef] [PubMed]
-
Bush A, Cole P, Hariri M, et al. Primary ciliary dyskinesia: diagnosis and standards of care. Eur Respir J. 1998; 12:982-988. [CrossRef] [PubMed]
-
Knowles MR, Daniels LA, Davis SD, et al. Primary ciliary dyskinesia. Recent advances in diagnostics, genetics, and characterization of clinical disease. Am J Respir Crit Care Med. 2013; 188:913-22. [CrossRef] [PubMed]
Reference as: Das D. Medical image of the week: Kartagener syndrome. Southwest J Pulm Crit Care. 2015;10(6):343-4. doi: http://dx.doi.org/10.13175/swjpcc057-15 PDF
Medical Image of the Week: Finger in Glove

Figure 1. PA (Panel A) and lateral (Panel B) chest x-ray showing finger in glove (arrow) in the right upper lung with other scattered areas of consolidation.

Figure 2. Repeat chest x-ray about a month later showing generalized clearing.
A 45-year old man with a history of asthma presented with increasing shortness of breath, and cough productive of dark firm plugs, sometimes branching. His chest x-ray (Figure 1) shows finger in glove (arrow) in the right upper lung with other scattered areas of consolidation. His serum IgE was elevated at 750 IU/ml (normal < 380 IU/ml). His eosinophil count was 12%. Aspergillus IgE was 6.69 (normal< 0.35). A diagnosis of probable allergic bronchopulmonary aspergillosis (ABPA) was made. He was given oral corticosteroids. Follow up about a month later showed dramatic clinical improvement and a repeat chest x-ray (Figure 2) showed generalized clearing.
The initial chest x-ray shows a “finger in glove” pattern in the right upper lobe (Figure 1, arrow), which is due to mucoid impaction within the larger bronchi (1). The same appearance has also been referred to as the rabbit ear appearance, Mickey Mouse appearance, toothpaste-shaped opacities, Y-shaped opacities, V-shaped opacities and the Churchill sign because it resembles the “V” gesture often associated with Winston Churchill.
ABPA is an immunological pulmonary disorder caused by hypersensitivity to Aspergillus fumigatus, manifesting with poorly controlled asthma, recurrent pulmonary infiltrates and central bronchiectasis (2). Primary therapy consists of oral corticosteroids to control exacerbations, itraconazole as a steroid-sparing agent and optimized asthma therapy. Uncertainties surround the prevention and management of bronchiectasis, chronic pulmonary aspergillosis and aspergilloma as complications, concurrent rhinosinusitis, environmental control and long-term management.
Gerald F. Schwartzberg, MD
Phoenix, AZ
References
- Weerakkody Y, Jones J. Finger in glove sign. Available at: http://radiopaedia.org/articles/finger-in-glove-sign (accessed 11/22/13).
- Agarwal R, Chakrabarti A, Shah A, Gupta D, Meis JF, Guleria R, Moss R, Denning DW; ABPA complicating asthma ISHAM working group. Allergic bronchopulmonary aspergillosis: review of literature and proposal of new diagnostic and classification criteria. Clin Exp Allergy. 2013;43(8):850-73. [CrossRef] [PubMed]
Reference as: Schwartzberg GF. Medical image of the week: finger in glove. Southwest J Pulm Crit Care. 2014:8(1):64-5. doi: http://dx.doi.org/10.13175/swjpcc169-13 PDF
December 2013 Imaging Case of the Month
Michael B. Gotway, MD
Department of Radiology
Mayo Clinic Arizona
Scottsdale, AZ
Clinical History
A 30-year-old man complained of intermittent shortness of breath and recurrent respiratory tract infections. Frontal chest radiography (Figure 1) was performed.
Figure 1. Frontal chest radiograph. Which of the following statements regarding the chest radiograph is most accurate?

Reference as: Gotway MB. December 2013 imaging case of the month. Southwest J Pulm Crit Care. 2013;7(6):339-47. doi: http://dx.doi.org/10.13175/swjpcc172-13 PDF
Medical Image of the Week: Kartagener Syndrome

Figure 1. Chest x-ray showing right-sided aortic knob, heart and stomach bubble (arrows).

Figure 2. Abdominal CT scan showing right-sided stomach bubble (white arrow) and left-sided liver (yellow arrow).


Figure 3. Representative thoracic CT lung windows showing bronchiectasis with bronchi larger than blood vessels with thickened bronchial walls (arrows).
A 52 year old woman was admitted for dyspnea and fatigue. Kartagener syndrome had been diagnosed at age 3 with situs inversus totalis (Figures 1 and 2). She has bronchiectasis (Figure 3) with chronic Pseudomonas colonization, chronic sinusitis, and nasal polyposis.
Kartagener syndrome is a type of primary cilia dyskinesia or immotile-cilia syndrome. When primary ciliary dyskinesia is combined with situs inversus it is known as Kartagener syndrome (KS) after the Swiss internist who recognized the association of situs inversus, bronchiectasis and sinusitis (1). It is popular in case presentations especially with the chest x-ray or CT scans deliberated presented inverted.
KS is an autosomal recessive disorder of the ciliary axoneme with incomplete penetrance and extensive heterogeneity (2). The typical ciliary axoneme consists of 2 central microtubules surrounded by 9 microtubular doublets. Patients with primary ciliary dyskinesia exhibit a wide range of defects in ciliary ultrastructure and motility, which ultimately impairs ciliary beating and mucociliary clearance. The most common defect is a reduction in the number of dynein arms, which decreases the ciliary beat frequency.
Treatment is similar to other forms of bronchiectasis and sinusitis. There is no definitive curative therapy.
Nam H. Chan MD, Robert W. Viggiano MD and Lewis J. Wesselius MD
Department of Pulmonary Medicine
Mayo Clinic Arizona
Scottsdale, AZ
References
- Kartagener M. Zur pathogenese der bronchiectasien. I Mitteilung:bronchiectasien bei situs viscerum inversus. Betr Klin Tuberk. 1933;83:498-501.
- Bent JP III, Willis EB. Kartagener syndrome. Medscape. Available at: http://emedicine.medscape.com/article/299299-overview (accessed 10/2/13).
Reference as: Chan NH, Viggiano RW, Wesselius LJ. Medical image of the week: Kartagener syndrome. Southwest J Pulm Crit Care. 2013;7(4):239-40. doi: http://dx.doi.org/10.13175/swjpcc137-13 PDF
June 2013 Imaging Case of the Month
Michael B. Gotway, MD
Department of Radiology
Mayo Clinic Arizona
Scottsdale, AZ
Clinical History
A 42-year-old woman complained of cough and intermittent wheezing with shortness of breath. Her previous medical history was unremarkable. Frontal and lateral (Figures 1A and B) chest radiography was performed.

Figure 1. Frontal (Panel A) and lateral (Panel B) chest x-ray.
Which of the following statements regarding the chest radiograph is most accurate?
- The chest radiograph shows no abnormalities
- The chest radiograph shows bilateral, basal reticulation suggesting fibrotic lung disease
- The chest radiograph shows medial left lower lobe opacities
- The chest radiograph shows large lung volumes associated with faint cystic change
- The chest radiograph shows numerous small nodules suggesting a miliary pattern
Reference as: Gotway MB. June 2013 imaging case of the month. Southwest J Pulm Crit Care. 2013;6(6):263-71. PDF
January 2012 Case of the Month
Michael B. Gotway, MD
Associate Editor Imaging
Clinical History
A 69-year-old woman with no significant past medical history presented with progressive shortness of breath. A chest radiograph (Figure 1) was obtained.

Figure 1. Frontal chest radiograph.
How would you describe the findings on the chest radiograph (Figure 1)?
Reference as: Gotway MB. January 2012 case of the month. Southwest J Pulm Crit Care 2012;4:12-18. (Click here for a PDF version)