
Imaging
Those who care for patients with pulmonary, critical care or sleep disorders rely heavily on chest radiology and pathology to determine diagnoses. The Southwest Journal of Pulmonary, Critical Care & Sleep publishes case-based articles with characteristic chest imaging and related pathology.
The editor of this section will oversee and coordinate the publication of a core of the most important chest imaging topics. In doing so, they encourage the submission of unsolicited manuscripts. It cannot be overemphasized that both radiologic and pathologic images must be of excellent quality. As a rule, 600 DPI is sufficient for radiographic and pathologic images. Taking pictures of plain chest radiographs and CT scans with a digital camera is strongly discouraged. The figures should be cited in the text and numbered consecutively. The stain used for pathology specimens and magnification should be mentioned in the figure legend. Those who care for patients with pulmonary, critical care or sleep disorders rely heavily on chest radiology and pathology to determine diagnoses. The Southwest Journal of Pulmonary, Critical Care & Sleep publishes case-based articles with characteristic chest imaging and related pathology. The editor of this section will oversee and coordinate the publication of a core of the most important chest imaging topics. In doing so, they encourage the submission of unsolicited manuscripts. It cannot be overemphasized that both radiologic and pathologic images must be of excellent quality. As a rule, 600 DPI is sufficient for radiographic and pathologic images. Taking pictures of plain chest radiographs and CT scans with a digital camera is strongly discouraged. The figures should be cited in the text and numbered consecutively. The stain used for pathology specimens and magnification should be mentioned in the figure legend.
August 2023 Imaging Case of the Month: Chew Your Food Carefully
Michael B Gotway MD1 and Yasmeen M Butt MD2
1Departments of Radiology and 2Laboratory Medicine, Division of Anatomic Pathology
Mayo Clinic-Arizona
Scottsdale, Arizona USA
History of Present Illness
A 50-year-old woman presents with a history of chronic dyspnea and cough, becoming particularly problematic following COVID-19 infection 4 months prior to presentation. While she did experience significant periodic oxygen desaturations during her COVID-19 infection, she was not hospitalized for this illness. The patient also reported wheezing in the previous few weeks.
Past Medical History, Family History and Social History
The patient’s past medical history was also notable for gastroesophageal reflux disease as well as both Coombs positive and iron deficiency anemia. She reports a history of asthma, well controlled with inhaler use.
The patient’s past surgical history included adenoidectomy, cholecystectomy, and gastric laparoscopic band placement.
Her medications included prednisone (20 mg daily), dextroamphetamine-amphetamine, furosemide, omeprazole, fluoxetine, zolpidem (Ambien), daily Bactrim, occasional Loratadine (Claritin). She also utilized an albuterol inhaler and Fluticasone-based (both Flonase and Breo Ellipta) inhalers.
The patient is a former smoker, ½ pack-per day for 26 years, having quit 11 years prior to presentation. She also reported a history of vaping (agent inhaled unclear) for 8 years, quitting 3 years earlier. She has no known allergies. She drinks alcohol socially and denied illicit drug use.
Physical Examination
The patient’s physical examination showed her temperature to be 99°F with normal pulse and respiratory rate but her blood pressure elevated at 160/90 mmHg. She was obese (263 lbs., BMI= 41). Bilateral basal rales were noted at her examination, but no other abnormal physical examination findings were detected.
Laboratory Evaluation
The patient’s room air pulse oximetry was 85%. A complete blood count showed an upper normal white blood cell count at 1.9 x109/L (normal, 4.5 – 11 x109/L). Her hemoglobin and hematocrit values were 10.7 gm/dL (normal, 12 – 16 gm/dL) and 37.1% (normal, 36 – 46%). The patient’s serum chemistries and liver function studies were entirely normal. The patient had an elevated anti-nuclear antibody titer at 1:320. An echocardiogram noted diastolic dysfunction but normal left ventricular contractility.
Frontal chest radiography (Figure 1) was performed.

Figure 1. Frontal chest radiography.
Which of the following statements regarding this chest radiograph is accurate? (Click on the correct answer to be directed to the second of 11 pages)
- Frontal chest radiography shows normal findings
- Frontal chest radiography shows marked cardiomegaly
- Frontal chest radiography shows mediastinal lymphadenopathy
- Frontal chest radiography shows pleural effusion
- Frontal chest radiography shows multifocal peribronchial consolidation
December 2021 Medical Image of the Month: Aspirated Dental Implant

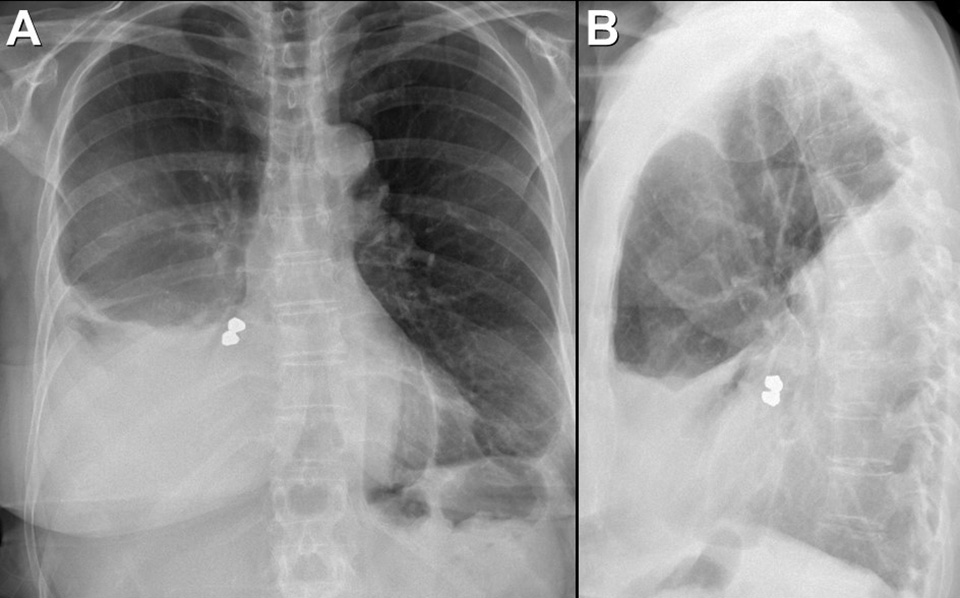
Figure 1. Frontal and lateral chest radiography shows right middle and lower lobe consolidation and a large right pleural effusion, suggesting pneumonia and parapneumonic effusion, but also shows a metallic focus in the right lower lobe. Click here to view Figure 1 enlarged in a new window.
{kind=link}

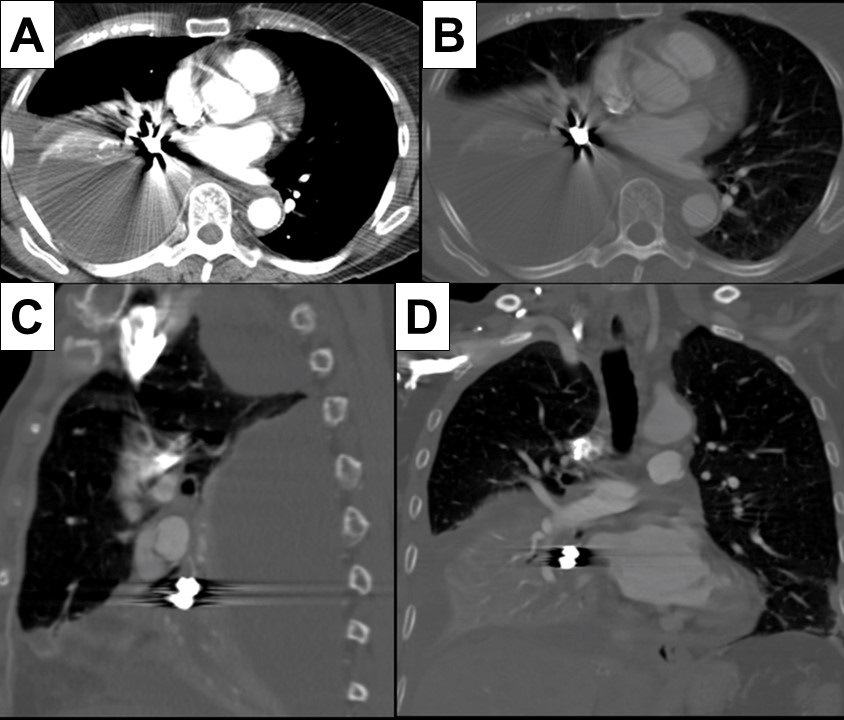
Figure 2. Axial (A and B), sagittal (C) and coronal (D) contrast-enhanced chest CT displayed in soft tissue (A) and bone (B-D) windows shows right lower lobe consolidation and loculated pleural effusion. A metallic focus closely related to the right lower lobe bronchus is present. Click here to view Figure 2 enlarged in a new window.
{kind=link}

Figure 3. Bronchoscopic images performed during retrieval of the right lower lobe foreign body shows a metallic object lodged within the right lower lobe bronchus. The object was retrieved using a forceps and found to represent a dental implant, evidently aspirated during the patient’s prolonged dental procedure. Click here to view Figure 3 enlarged in a new window.
{kind=link}
A 76-year-old woman with a past medical history significant for left-sided breast cancer status post lumpectomy recently underwent an extensive dental procedure about 1 month prior to presentation. The dental procedure was prolonged, and the patient reported falling asleep during the procedure several times. She presented with fatigue, right pleuritic chest pain, low-grade fevers, and drenching sweats. She underwent chest radiography at an outside institution which disclosed pneumonia, for which she was treated with cefdinir and doxycycline without improvement. Thoracostomy tube drainage of the pleural effusion was performed and showed empyema. Imaging showed an airway foreign body which was retrieved bronchoscopically. The patient made an uneventful recovery.
Aspiration during dental procedures is rare but reported (1). Dental items have been reported as the second most commonly ingested/aspirated foreign objects in adults. If the airway is not compromised, assessment for any lost or missing instrument and its component should be done promptly with a high suspicion of mishap. Fortunately, many dental appliances and instruments are often, but not always, radiopaque and may be detected by chest radiography. Many can be removed by bronchoscopy, as in this case.
Prasad M. Panse MD1, Sreeja Biswas Roy MD2, Robert W. Viggiano MD2
Departments of Radiology1 and Pulmonary Medicine2
Mayo Clinic Arizona
Scottsdale, AZ USA
Reference
- Yadav RK, Yadav HK, Chandra A, Yadav S, Verma P, Shakya VK. Accidental aspiration/ingestion of foreign bodies in dentistry: A clinical and legal perspective. Natl J Maxillofac Surg. 2015; 6(2):144-1451. [CrossRef] [PubMed]
Cite as: Panse PM, Biswas Roy S, Viggiano RW. December 2021 Medical Image of the Month: Aspirated Dental Implant. Southwest J Pulm Crit Care. 2021;23(6):149-50. doi: https://doi.org/10.13175/swjpcc040-21 PDF
Medical Image of the Month and Brief Review: Aspiration Pneumonia in an Intubated Patient with COVID-19

Figure 1. Severe aspiration changes on CT. Bronchial wall thickening (white arrow) could barely be perceived elsewhere given the dense layering secretions (black arrows) in bilateral mainstem bronchi and filling the dependent segmental bronchi. Atelectatic collapse (black arrowhead) can be seen distal to the obstructed bronchi. Rounded consolidation (white arrowhead) as seen later in the course of SARS2 COVID-19.
A woman in her 60’s likely acquired COVID-19 through community transmission. When she developed respiratory distress, she came to the emergency department, was found to have abnormalities on chest x-ray and was intubated, testing positive on COVID-19 PCR. She developed worsening hypoxia over the course of one night after a fairly stable ICU course. CT was obtained and demonstrated severe aspiration changes including bronchial filling and collapse of the dependent lower lobes. Increased attention to suctioning helped with the desaturations, and she eventually recovered and was extubated. This case serves as a reminder to ensure adequate suctioning while patients are intubated to prevent aspiration, obstruction and related ventilator-associated pneumonia.
Discussion
Aspiration is a relatively common event which typically resolves with no clinical sequelae. In fact, recent studies have estimated that up to 50% of healthy adults aspirate while in their sleep (1). Pulmonary symptoms of aspiration generally only occur when there is compromise to the usual defenses that protect the lower airways (cough reflex, glottis closure, etc.) and when an inoculum is introduced which has a direct toxic effect on the lower airways, resulting in inflammation. Common predisposing conditions which can lead to aspiration include reduced consciousness (commonly seen in patients with alcohol abuse or IV drug use), dysphagia from neurologic deficits, disorders of the upper GI tract, or mechanical disruption of glottis closure due to endotracheal intubation, bronchoscopy, endoscopy, or NG feeding (2,3). Endotracheal intubation is a key risk factor in ventilator associated pneumonia (4). This brief review will focus on ventilator-associated pneumonia.
Overview and epidemiology: Ventilator-associated pneumonia is defined as new onset pneumonia at least 48 hours following intubation. Despite being frequently thought of as partially protective, the presence of an endotracheal tube may actually serve as a mechanism of transport of organisms from the oropharyngeal tract (most commonly) or GI tract (less commonly) to the lung (5,6). Recent data from 2012 to 2013 suggest that the percentage of patients on ventilator support who go on to acquire aspiration pneumonia is 9.7% (7). Common pathogens associated with this condition include aerobic gram-negative bacilli (Escherichia coli, Klebsiella pneumoniae, Enterobacter spp, Pseudomonas aeruginosa, Acinetobacter spp) or gram-positive cocci including MRSA and Streptococcus Pneumoniae.
Prevention: Patients should be placed in the semi-recumbent position (45 degrees) and have intermittent (every 3-6 hours) or continuous subglottic drainage (8,9). Studies have found there isn’t a significant difference in clinical outcomes between intermittent and continuous drainage and that intermittent drainage may be associated with less adverse effects (10). The use of acid reducing agents should also be avoided, although sucralfate use decreased ICU-acquired pneumonia (11). Gastric volume monitoring had long been the standard of clinical practice with an aim to prevent vomiting and subsequent aspiration, however recent studies have suggested that gastric volume monitoring correlates poorly with aspiration risk and may lead to a decrease in caloric delivery (12,13).
Symptoms/Signs
- Important signs include fever, tachypnea, increased purulent secretions or hemoptysis; systemic signs including encephalopathy or sepsis may also be present (12).
- Ventilator: Reduced tidal volume, increased inspiratory pressures
- Labs: worsening hypoxemia, leukocytosis
- Imaging:
- New or progressive infiltrates on CXR commonly with alveolar infiltrates or silhouetting of adjacent solid organs
- Air bronchograms are common
Treatment
Empiric treatment choices should be guided by local distribution of pathogens and susceptibility of those pathogens to antimicrobials (14-16). Treatment options should also take into consideration the likelihood of MDR organisms or MRSA. In a meta-analysis of 15 studies, factors associated with an increased risk of MDR VAP were IV antibiotics in the last 90 days, >5 days of hospitalization prior to onset of symptoms, septic shock on presentation of VAP, ARDS before VAP, and renal replacement therapy prior to VAP. Risk factors for MRSA include treatment in units where >10 to 20% of S. Aureus isolates are methicillin resistant, treatment in a unit where prevalence of MRSA is not known, or prior history of MRSA infection. In the absence of risk factors for MDR or MRSA, patients with VAP should receive one agent that has activity against Pseudomonas, other gram-negative bacilli, and MSSA. Patients with risk factors for MDR or MRSA should receive two agents with activity against P. Aeruginosa and other gram-negative bacilli and one agent with activity against MRSA (15). An algorithm guiding specific regimens for treatment of VAP can be found on UpToDate’s article: Treatment of hospital-acquired and ventilator-associated pneumonia in adults (17).
Jeremy P. Head BS and Michael C. Larson MD
Department of Medical Imaging
University of Arizona
Tucson, AZ USA
References
- Huxley EJ, Viroslav J, Gray WR, Pierce AK. Pharyngeal aspiration in normal adults and patients with depressed consciousness. Am J Med. 1978;64(4):564-568. [CrossRef] [PubMed]
- Lo WL, Leu HB, Yang MC, Wang DH, Hsu ML. Dysphagia and risk of aspiration pneumonia: A nonrandomized, pair-matched cohort study. J Dent Sci. 2019;14(3):241-247. [CrossRef] [PubMed]
- Mandell LA, Niederman MS. Aspiration Pneumonia. N Engl J Med. 2019;380(7):651-663. [CrossRef] [PubMed]
- Rouzé A, Jaillette E, Nseir S. Relationship between microaspiration of gastric contents and ventilator-associated pneumonia. Ann Transl Med. 2018;6(21):428. [CrossRef] [PubMed]
- Garrouste-Orgeas M, Chevret S, Arlet G, et al. Oropharyngeal or gastric colonization and nosocomial pneumonia in adult intensive care unit patients. A prospective study based on genomic DNA analysis. Am J Respir Crit Care Med. 1997;156(5):1647-1655. [CrossRef] [PubMed]
- Jaillette E, Girault C, Brunin G, et al. Impact of tapered-cuff tracheal tube on microaspiration of gastric contents in intubated critically ill patients: a multicenter cluster-randomized cross-over controlled trial. Intensive Care Med. 2017;43(11):1562-1571. [CrossRef] [PubMed]
- Metersky ML, Wang Y, Klompas M, Eckenrode S, Bakullari A, Eldridge N. Trend in Ventilator-Associated Pneumonia Rates Between 2005 and 2013. JAMA. 2016;316(22):2427-2429. [CrossRef] [PubMed]
- Wang L, Li X, Yang Z, et al. Semi-recumbent position versus supine position for the prevention of ventilator-associated pneumonia in adults requiring mechanical ventilation. Cochrane Database Syst Rev. 2016;2016(1):CD009946. [CrossRef] [PubMed]
- Caroff DA, Li L, Muscedere J, Klompas M. Subglottic Secretion Drainage and Objective Outcomes: A Systematic Review and Meta-Analysis. Crit Care Med. 2016;44(4):830-840. [CrossRef] [PubMed]
- Mao Z, Gao L, Wang G, et al. Subglottic secretion suction for preventing ventilator-associated pneumonia: an updated meta-analysis and trial sequential analysis. Crit Care. 2016;20(1):353. Published 2016 Oct 28. [CrossRef] [PubMed]
- Alquraini M, Alshamsi F, Møller MH, et al. Sucralfate versus histamine 2 receptor antagonists for stress ulcer prophylaxis in adult critically ill patients: A meta-analysis and trial sequential analysis of randomized trials. J Crit Care. 2017;40:21-30. [CrossRef] [PubMed]
- Meduri GU. Diagnosis and differential diagnosis of ventilator-associated pneumonia. Clin Chest Med. 1995;16(1):61-93. [PubMed]
- McClave SA, Lukan JK, Stefater JA, et al. Poor validity of residual volumes as a marker for risk of aspiration in critically ill patients. Crit Care Med. 2005;33(2):324-330. [CrossRef] [PubMed]
- Kalil AC, Metersky ML, Klompas M, et al. Executive Summary: Management of Adults With Hospital-acquired and Ventilator-associated Pneumonia: 2016 Clinical Practice Guidelines by the Infectious Diseases Society of America and the American Thoracic Society [published correction appears in Clin Infect Dis. 2017 May 1;64(9):1298] [published correction appears in Clin Infect Dis. 2017 Oct 1;65(7):1251]. Clin Infect Dis. 2016;63(5):575-582. [CrossRef] [PubMed]
- Beardsley JR, Williamson JC, Johnson JW, Ohl CA, Karchmer TB, Bowton DL. Using local microbiologic data to develop institution-specific guidelines for the treatment of hospital-acquired pneumonia. Chest. 2006;130(3):787-793. [CrossRef] [PubMed]
- Jones RN. Microbial etiologies of hospital-acquired bacterial pneumonia and ventilator-associated bacterial pneumonia [published correction appears in Clin Infect Dis. 2010 Nov 1;51(9):1114]. Clin Infect Dis. 2010;51 Suppl 1:S81-S87. [CrossRef] [PubMed]
- Klompas M. Treatment of hospital-acquired and ventilator-associated pneumonia in adults. UpToDate. July 31, 2020. Available at: https://www.uptodate.com/contents/treatment-of-hospital-acquired-and-ventilator-associated-pneumonia-in-adults (requires subscription).
Cite as: Head JP, Larson MC. Medical image of the month and brief review: aspiration pneumonia in an intubated patient with COVID-19. Southwest J Pulm Crit Care. 2020;21(2):35-8. doi: https://doi.org/10.13175/swjpcc040-20 PDF
Medical Image of the Week: Barium Aspiration

Figure 1: Upright X-Ray of the chest showing dense opacifications in the bilateral lower lobes consistent with Barium Aspiration.
An 88-year old man was referred for video fluoroscopic swallow study (VFSS) for concerns of aspiration as the cause of his chronic cough. As part of the study, he was given barium sulfate nectar which he aspirated and developed respiratory distress and hypoxia requiring hospital admission. Chest X-ray obtained at that time is shown (Figure 1).
Although inert, acute inflammation and even death attributed to barium aspiration has been described (1,2). Severe respiratory complications tend to occur in patients with extensive comorbidities (2,3). Treatment is mostly supportive and severe cases may require invasive ventilatory support. Bronchoscopy and suction clearance may be attempted although the success is variable. Recovery is usually complete although fibrosis is a known complication (4).
Bhupinder Natt, MD
Division of Pulmonary, Allergy, Critical Care and Sleep
Banner-University Medical Center
Tucson, AZ USA
References
- Kaira K, Takise A, Goto T, Horie T, Mori M. Barium sulphate aspiration. Lancet 2004;364(9452):2220. [CrossRef] [PubMed]
- Gray C, Sivaloganathan S, Simpkins KC. Aspiration of high density barium contrast medium causing acute pulmonary inflammation- report of two fatal cases in elderly women with disordered swallowing. Clinic Radiol. 1989;40(4):397-400. [CrossRef] [PubMed]
- Fruchter O, Dragu R. Images in Clinical Medicine. A deadly examination. N Engl J Med. 2003;348(11):1016. [CrossRef] [PubMed]
- Voloudaki A, Ergazakis N, Gourtsoyiannis N. Late changes in barium sulfate aspiration. HRCT Features. Eur Radiol. 2003;13(9):2226-9. [CrossRef] [PubMed]
Cite as: Natt B. Medical image of the week: barium aspiration. Southwest J Pulm Crit Care. 2017;15(6): . doi: https://doi.org/10.13175/swjpcc146-17 PDF
October 2017 Imaging Case of the Month
Paul J. Conomos, MD1
Michael B. Gotway, MD2
1Arizona Pulmonary Specialists
Phoenix, AZ USA
2Mayo Clinic Arizona
Scottsdale, AZ USA
Clinical History: An 18-year-old man with no known previous medical history presented with complaints of intermittent cough persisting several months. No hemoptysis was noted.
Physical examination was largely unremarkable and the patient’s oxygen saturation was 99% on room air. The patient’s vital signs were within normal limits.
Laboratory evaluation was unremarkable. Quantiferon testing for Mycobacterium tuberculosis was negative, and testing for coccidioidomycosis was unrevealing. Frontal and lateral chest radiography (Figure 1) was performed.

Figure 1. Figure 1. Frontal (A) and lateral (B) chest radiography.
Which of the following statements regarding the chest radiograph is most accurate? (Click on the correct answer to proceed to the second of eight pages)
- The chest radiograph shows asymmetric reticulation and interlobular septal thickening
- The chest radiograph shows bilateral reticulation associated with decreased lung volumes
- The chest radiograph shows focal consolidation
- The chest radiograph shows large lung volumes
- The chest radiograph shows small cavitary pulmonary nodules
Cite as: Conomos PJ, Gotway MB. October 2017 imaging case of the month. Southwest J Pulm Crit Care. 2017;15(4):138-46. doi: https://doi.org/10.13175/swjpcc119-17 PDF
August 2017 Imaging Case of the Month
Brandon T. Larsen, MD, PhD1
Michael B. Gotway, MD2
Departments of Pathology1 and Radiology2
Mayo Clinic Arizona
Scottsdale, Arizona USA
Clinical History: A 67-year-old man with a 23 pack-year history of smoking, stopping 6 years earlier, presented with a year-long history of intermittent hemoptysis consisting of small specs of blood particularly in the morning after he awoke. No sputum discoloration was reported and the patient denied shortness of breath, fever, shortness of breath, and chills. The patient also denied rash, joint pain, and night sweats. His past surgical history was remarkable only for an appendectomy, tonsillectomy, and repair of an ankle fracture, all as a young man. The patient did report some asbestos exposure in the past. He takes a multivitamin and occasional over-the counter pain relievers, but was not taking prescription medications.
Physical examination: unremarkable and the patient’s oxygen saturation was 98% on room air.
Laboratory evaluation: largely unremarkable. Quantiferon testing for Mycobacterium tuberculosis was negative. An outside otolaryngology examination was reported to show no abnormalities. Frontal chest radiography (Figure 1) was performed.

Figure 1. Frontal chest radiography.
Which of the following statements regarding the chest radiograph is most accurate? (Click on the correct answer to proceed to the second of nine pages)
- The chest radiograph shows a mediastinal mass
- The chest radiograph shows multifocal consolidation and pleural effusion
- The chest radiograph shows multifocal smooth interlobular septal thickening
- The chest radiograph shows a possible focal air space opacity
- The chest radiograph shows small cavitary pulmonary nodules
Cite as: Larsen BT, Gotway MB. August 2017 imaging case of the month. Southwest J Pulm Crit Care. 2017;15(2):69-79. doi: https://doi.org/10.13175/swjpcc098-17 PDF
Medical Image of the Week: Zenker’s Diverticulum

Figure 1. Panel A: PA view chest x-ray shows possible cavitation with air-fluid level in the right upper lobe (arrow). Panel B: lateral view chest x-ray shows possible cavitation with air-fluid level in the right upper lobe (arrow).

Figure 2. Coronal section of the thoracic CT scan shows focal dilation of the upper thoracic esophagus which contains fluid (arrow).

Figure 3. Endoscopic view of the upper esophagus showing the diverticulum with impacted food bolus.
A 71-year-old man with history of recurrent aspiration pneumonia and previous esophageal surgery presented to the Emergency Department with acute hypoxia and leukocytosis. Imaging, above, showed a consolidation in the RUL and on lateral view an air fluid level. This was suspicious for infection or malignancy. For the ongoing concern for possible esophageal pathology given previous surgery, GI was consulted and upper endoscopy performed. He was found to have an esophageal dilation at repair site of a previous Zenker’s diverticulum filled with food.
Zenker’s Diverticulum is a defect in the muscular wall of the hypopharynx in an area known as Killian's triangle. This condition is male predominant mainly occurring in the 3rd to 4th decade and/or the 7th to 8th decade of life. The out pouching created will accumulate food and eventually lead to high incidences of aspiration pneumonia. Treatment is usually surgical in nature and can cause vocal cord damage and even recurrence of the outpouching (1).
Chandra Stockdall MD and Roberto Swazo MD
Department of Internal Medicine
Banner University Medical Center South Campus
Tucson, AZ USA
Reference
- Mulder C, Van Delft F. Zenker’s diverticulum. UpToDate. May, 2017. Available at: http://www.uptodate.com/contents/zenkers-diverticulum (requires subscription, accessed 6/30/17).
Cite as: Stockdall C, Swazo R. Medical image of the week: Zenker's diverticulum. Southwest J Pulm Crit Care. 2017;15(1):15-6. doi: https://doi.org/10.13175/swjpcc075-17 PDF
Medical Image of the Week: Papillomatosis

Figure 1. Chest roentgenogram.

Figure 2. Contrast enhanced computer tomography of chest.
A 24-year-old man with recurrent respiratory papillomatosis presented with a history of breathlessness and a change in voice for the last four months. He had undergone endoscopic debridement in the past for laryngeal papillomatosis. On initial evaluation, respiratory distress was thought to be due to recurrence of laryngeal papillomatosis as he improved after surgical de-bulking of laryngo-tracheal papillomas. However, he had some trickle of blood into bronchi with debridement under general anaesthesia. Post-operative chest roentgenogram showed bilateral patchy opacities giving the appearance of aspiration pneumonitis as shown in figure 1.
He also underwent contrast enhanced computer tomography of the chest which showed numerous but small cavitary lesions involving bilateral lung parenchyma as shown in figure 2. This lead to the diagnosis of pulmonary spread of laryngeal papillomatosis and the patient was given adjuvant treatment for this aggressive disease (1,2).
K Devaraja, MS, DNB and Kapil Sikka, MS, DNB
All India Institute of Medical Sciences
Ansari Nagar, New Delhi, India
References
- Abe K, Tanaka Y, Takahashi M, Kosuda S, et al. Pulmonary spread of laryngeal papillomatosis: radiological findings. Radiat Med. 2006 May;24(4):297–301. [CrossRef] [PubMed]
- Carifi M, Napolitano D, Morandi M, Dall'Olio D. Recurrent respiratory papillomatosis: current and future perspectives. Ther Clin Risk Manag. 2015;11:731–8. [CrossRef] [PubMed]
Cite as: Devaraja K, Sikka K. Medical image of the week: papillomatosis. Southwest J Pulm Crit Care. 2017;14(3):123-4. doi: https://doi.org/10.13175/swjpcc025-17 PDF
Medical Image of the Week: Tracheobronchial Foreign Body Aspiration

Figure 1. Panel A: The chest x-ray failed to show the aspirated foreign body. Panels B and C: Flexible bronchoscopy was performed and the insulin syringe cap was visualized in the right mainstem bronchus and retrieved with forceps.

Figure 2. Panel A: CT chest shows interval development of ground glass opacities and air fluid level in the right middle lobe (arrow). Panel B: The foreign body is visualized in the right lower lobe bronchus as an endobronchial-filling defect (arrow). Panel C: Flexible bronchoscopy was performed and cashew piece was retrieved with suction.
Case 1 (Figure 1) is a 58-year-old man who accidentally inhaled his insulin syringe cap while swinging on his recliner with the cap perched in his mouth. He developed a dry irritating cough. On exam he had mild stridor in the upper airways and bilateral wheezing. The insulin cap was visualized by bronchoscopy in the right mainstem bronchus and retrieved with forceps.
Case 2 (Figure 2) is a 65-year-old man with chronic dysphagia and poor dentition who choked on a cashew. It took repeated coughing attempts to produce the cashew, but it was unclear whether the entire content was cleared. He then developed non-massive hemoptysis that persisted for 2 weeks. Thoracic CT showed ground glass opacities and an air fluid level in the right middle lobe. The foreign body was visualized in the right lower lobe bronchus as an endobronchial-filling defect. Bronchoscopy revealed a cashew piece in the right lower lobe bronchus. Forceps trials failed due to fragility of the foreign body, which was ultimately retrieved with scope suction.
Rigid bronchoscopy is the gold standard for diagnosis and management of tracheobronchial foreign body aspiration, but flexible bronchoscopy is another accepted method that is also more comfortable for the patient (1). Virtual bronchoscopy is a noninvasive procedure that can assist with localizing the foreign body and may have a role to play in follow-up assessment of airway patency (2). Pneumonia and atelectasis are common complications. Less common complications include bronchiectasis, bronchostenosis, hemoptysis, tracheal perforation, pneumomediastinum, and even cardiopulmonary arrest (3). Tracheal foreign bodies pose more danger than bronchial foreign bodies; in such cases the foreign body should be pushed to distal airways, crumbled if it is organic, and then extracted (1).
Khushboo Goel, MD1, Huthayfa Ateeli, MBBS2, Joshua Dill, DO2, Dena L’Heureux MD3
1Department of Internal Medicine, University of Arizona, Tucson, AZ, USA
2Department of Internal Medicine, Division of Pulmonary, Critical Care, Sleep, and Allergy Medicine, University of Arizona, Tucson, AZ, USA
3Department of Internal Medicine, Division of Pulmonary, Critical Care, and Sleep Medicine, Southern Arizona VA Health Care System, Tucson, AZ, USA
References
- Altunas B, Aydin Y, Eroglu A. Foreign bodies in trachea: a 25 year experience. Eurasian J Med. 2016;48(2):119-123. [CrossRef] [PubMed]
- Kshatriya RM, Khara NV, Paliwal RP, Patel SN. Role of virtual and flexible bronchoscopy in the management of a case of unnoticed foreign body aspiration presented as a nonresolving pneumonia in an adult female. Lung India. 2016; 33(4):420-423. [CrossRef] [PubMed]
- Altunas B, Aydin Y, Eroğlu A. Complications of tracheobronchial foreign bodies. Turk J Med Sci. 2016;46(3):785-800. [CrossRef] [PubMed]
Cite as: Goel K, Ateeli H, Dill J, L’Heureux D. Medical image of the week: tracheobronchial foreign body aspiration. Southwest J Pulm Crit Care. 2016;13(4):184-5. doi: http://dx.doi.org/10.13175/swjpcc092-16 PDF
Medical Image of the Week: Healthcare-associated Pneumonia Secondary to Aspiration

Figure 1. Panel A: Axial computed-tomography image demonstrating a foreign body within the right main-stem bronchus, with consolidation and volume loss of right lung. Panel B: Coronal view.

Figure 2. Panel A: bronchoscopy revealing an ingested foreign body in the right main-stem bronchus. Panel B: forceps retrieval yielded a large piece of broccoli.
A 57 year-old bedbound paraplegic man developed a worsening productive cough after being hospitalized for several days. He was brought to the radiology suite for a CT scan of the chest, revealing a soft tissue density within his right main-stem bronchus, with volume loss of his right lung (Figure 1). Bronchoscopy was performed, yielding a 2 cm piece of broccoli, successfully removed with forceps (Figure 2). Culture from the bronchial aspirate was positive for Pseudomonas aeruginosa. The patient’s respiratory status dramatically improved after removal of the foreign body and commencement of pathogen-directed antibiotics. This study illustrates a dramatic example of healthcare-associated pneumonia (HCAP) secondary to aspiration, as described by the American Thoracic Society / Infectious Diseases Society of America (1).
Lavi Nissim MD, Sam Alnajjar MD and Edward Vivio RT
Phoenix Baptist Hospital
2000 W. Bethany Home Road
Phoenix, AZ 85015
Reference
- American Thoracic Society; Infectious Diseases Society of America. Guidelines for the management of adults with hospital-acquired, ventilator-associated, and healthcare-associated pneumonia. Am J Respir Crit Care Med. 2005;171(4):388-416. [CrossRef] [PubMed]
Reference as: Nissim L, Alnajjar S, Vivio E. Medical image of the week: healthcare-associated pneumonia secondary to aspiration. Southwest J Pulm Crit Care. 2015;11(1):1-2. doi: http://dx.doi.org/10.13175/swjpcc065-15 PDF
April 2015 Imaging Case of the Month
Michael B. Gotway, MD
Department of Radiology
Mayo Clinic Arizona
Scottsdale, AZ
Clinical History: A 73-year-old woman with a history of ovarian malignancy in remission for several years and treated with hysterectomy and oopherectomy, hypothyroidism, and hypertension, presented with rather abrupt onset cough, chest pain, dyspnea and low-grade fever (99.6°F). Her past medical history was otherwise unremarkable. Her medications included thyroid replacement, amlodipine, benazepril, and, recently, calcium and magnesium supplementation. Chest radiography was performed (Figure 1).

Figure 1. Frontal (panel A) and lateral (panel B) chest radiographs.
Which of the following statements regarding the chest radiograph is most accurate? (Click on the correct answer to proceed to the second of nine panels)
Reference as: Gotway MB. April 2015 imaging case of the month. Southwest J Pulm Crit Care. 2015;10(4):171-81. doi: http://dx.doi.org/10.13175/swjpcc048-15 PDF
Medical Image of the Week: Killian-Jamieson Diverticulum

Figure 1. Chest x-ray showing worsening consolidation in both lungs.

Figure 2. Anterior (panel A) and lateral (panel B) fluoroscopic images showing retained contrast material in the anterior esophageal diverticulum in the hypopharynx.
An 89 year old female nursing home resident with a past medical history of hypertension and coronary artery disease was admitted with generalized weakness and vomiting for two days. Chest x-ray revealed consolidation in the left lung suggestive of pneumonia and she was started on broad spectrum antibiotics. Due to worsening consolidation in both lung fields (Figure 1) a video swallow was done for possible aspiration, which revealed contrast retained within the proximal esophagus within a diverticula in the anterior aspect (Figure 2). After excision of the diverticulum her pneumonia resolved and she was discharged back to the nursing home.
Killian-Jamieson diverticulum is a mucosal protrusion through a muscular gap in the anterolateral wall of the cervical esophagus; inferior to the cricopharyngeus and lateral to the longitudinal muscle of the esophagus just below its insertion on the posterior lamina of cricoid cartilage (gap also known as Killian-Jamieson space). This differentiates it from the Zenker’s diverticulum which arises from the muscular gap in the posterior portion of cricopharyngeus muscle (also known as Killian’s dehiscence). Killian-Jamieson diverticulum causes more non-specific symptoms than Zenker's diverticulum. Because these diverticula occur in close proximity to the recurrent laryngeal nerve, it should be carefully preserved during surgical resection.
Chandramohan Meenakshisundaram, MD and Nanditha Malakkla, MD
Medical Education
Saint Francis Hospital
Evanston, IL
References
- Kim DC, Hwang JJ, Lee WS, Lee SA, Kim YH, Chee HK. Surgical treatment of killian-jamieson diverticulum. Korean J Thorac Cardiovasc Surg. 2012;45(4):272-4. [CrossRef] [PubMed]
- Siddiq MA, Sood S, Strachan D. Pharyngeal pouch (Zenker's diverticulum). Postgrad Med J. 2001;77:506-11. [CrossRef] [PubMed]
- Brant WE, Helms CA. Fundamentals of Diagnostic Radiology. Lippincott Williams & Wilkins. (2007) ISBN:0781765188
Reference as: Meenakshisundaram C, Malakkla N. Medical image of the week: killian-jamieson diverticulum. Southwest J Pulm Crit Care. 2014;9(5):287-8. doi: http://dx.doi.org/10.13175/swjpcc134-14 PDF
Medical Image of the Week: Pneumatocele

Figure 1. Portable AP film showing a large cystic lesion in the left lower lobe in addition to small bilateral pleural effusions and adjacent consolidation.

Figure 2. Axial enhanced CT scan section showing a large cystic space with an air-fluid level with adjacent consolidated atelectasis. No perceptible wall is seen.
A 50-year-old man presented with polymicrobial pneumonia which included Proteus mirabilis, Enterobacter cloacea and MRSA pathogens. A large cystic lesion with an air-fluid level was found on chest imaging in a region of pneumonia (Figure 1). There was associated mass effect onto the adjacent lung. No perceptible wall was noted which would be more associated with a cyst rather than a cavity or abscess. Directed aspiration of this lesion resulted in decompression without further complication. Minimal sterile fluid was recovered. Therefore the proposed diagnosis was a pneumatocele within the setting of infection. Pneumatoceles may be challenging at times to distinguish from a cavity particularly when surrounded by airspace disease however merit consideration in the differential diagnosis particularly in the absence of findings of a thick irregular wall.
The exact mechanism causing development of a pneumatocele is not known, but believed to develop due to a check valve type bronchiole or bronchiolar obstruction (1). Pneumatoceles most commonly undergo spontaneous remission within weeks to months without any known long term implications. Complications occur rarely and include pneumothorax, tension pneumatocele, and secondary infection of a pneumatocele. Usual treatment is directed towards the underlying pneumonia with appropriate antibiotics. In rare cases percutaneous drainage may be necessary and is ideally performed with a small bore catheter to minimize trauma. The role of positive pressure ventilation in development of a pneumatocele is unclear.
Bhupinder Natt, MD and Veronica Arteaga, MD
Divisions of Pulmonary and Thoracic Imaging
University of Arizona College of Medicine
Tucson, AZ
Reference
- Lysy J, Werczberger A, Globus M, Chowers I. Pneumatocele formation in a patient with Proteus mirabilis pneumonia. Postgrad Med J. 1985;61(713):255-7. [CrossRef] [PubMed]
Reference as: Natt B, Arteaga V. Medical image of the week: pneumatocele. Southwest J Pulm Crit Care. 2014;9(2):126-7. doi: http://dx.doi.org/10.13175/swjpcc102-14 PDF